Abstract
The force required to fracture the temporal bone is substantial and can lead to vascular injury, hearing loss, vertigo or imbalance, facial nerve injury, and cerebral spinal fluid leaks. Various classification schemes have been proposed, with those identifying critical structures being more useful. CT remains the imaging modality of choice. Hearing loss remains the most common complication while facial nerve paralysis continues to be one of the most dreaded consequences. This chapter discusses the epidemiology of temporal bone trauma, the pathophysiology as well as complications, and current recommendations in management.
Keywords
temporal bone fracture, hearing loss, facial nerve paralysis, vertigo
The force required to fracture the temporal bone is substantial and can lead to vascular injury, hearing loss, vertigo or imbalance, facial nerve injury, and cerebral spinal fluid (CSF) leaks. This chapter will discuss the epidemiology of temporal bone trauma, the pathophysiology as well as complications, and current recommendations for management.
Etiology
Motor vehicle collisions (MVCs) are the primary mechanism of injury, followed by assaults, falls, and gunshot wounds (GSWs). Falls and violence are making up an increasing proportion of injuries. A recent series found that falls accounted for the majority of injuries, while in another series, violence was estimated to be as high as 70%. Among children, mechanisms include falls, crush or blunt injuries, MVCs, and GSWs.
Approximately 1875 lb of force is required to fracture the temporal bone. Transverse fractures caused by frontal or occipital forces require more energy than longitudinal fractures that occur with lateral force. Fractures associated with GSWs occur at far lower energies (0.3 kJ) than with falls (5 kJ). Damage from a GSW is dependent on the projectile’s kinetic energy, the weapon’s caliber, and the plasticity of the bullet. Low-velocity projectiles deflect off of bone, leading to non-linear and unpredictable paths, while high-velocity projectiles penetrate bone, leading to crush injuries and cavity formation.
Temporal Bone Anatomy
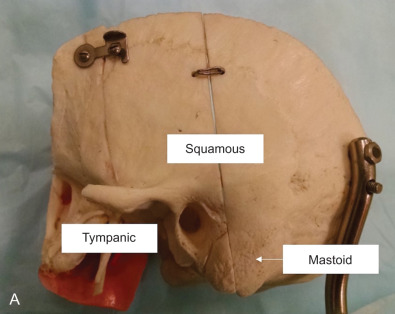
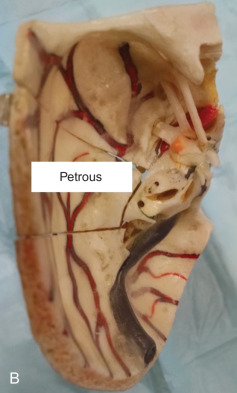
The temporal bone consists of the squamous, petrous, tympanic and mastoid portions ( Fig. 1.17.1 ). The squamous portion articulates with the frontal, parietal, and occipital bones to form the lateral skull. The petrous bone is wedge-shaped, extending anteromedially, and contains the otic capsule (OC), carotid canal, and facial nerve. The tympanic ring abuts the petrous portion and is posterior to the mandibular condyle. The mastoid portion contains the vertical facial nerve.
Clinical Presentation
History and Physical Examination
A complete head and neck exam is performed to confirm airway stability, neurological status, soft tissue injury, craniofacial fractures, and cranial nerve status. Life-threatening injuries are addressed first. Mortality in these individuals is 10%. Almost half report loss of consciousness (LOC) and in children, LOC, altered mental status (AMS), headache, and nausea/vomiting are common findings. Intracranial injuries are seen in up to 79% of temporal bone fractures. Common injuries include subdural hematoma and subarachnoid hemorrhage, with 17%–30% of patients requiring surgical neurological intervention.
Hemotympanum, hearing loss, vertigo, and nystagmus are strong predictors of temporal bone fractures. Other suggestive findings include external auditory canal (EAC) lacerations, otorrhagia, and tympanic membrane (TM) perforation. Classically, the examiner may appreciate ecchymosis over the mastoid tip (“Battle’s sign”), hemotympanum or periorbital ecchymosis (“raccoon eyes”).
Otorrhagia is common, and the presence of a “halo sign” (clear fluid ring external to internal blood ring when ear fluid drains onto filter paper) can signal a leak of cerebrospinal fluid (CSF). Significant bleeding can indicate a carotid injury. Prompt packing, imaging, and consultation with vascular surgery, interventional neuroradiology, or neurosurgery are necessary.
Presence of nystagmus can suggest OC trauma. The direction of the nystagmus can provide a clue as to which labyrinth may be affected with nystagmus beating towards the intact ear. Once the patient’s C-spine is cleared, head impulse testing to assess semicircular canal function and Dix–Hallpike testing for benign paroxysmal positioning vertigo (BPPV) are performed. Presence of direction changing, pendular, or vertical nystagmus that does not suppress with visual input may suggest central findings and should be further investigated.
As soon as the patient is cooperative, a facial nerve exam should be consistently documented. It is critical that each of the five branches of the facial nerve is examined. Temporal bone fractures generally affect all five branches of the facial nerve, and examination should note the degree of brow elevation, eye closure (minimal and maximal effort), nasal ala flaring/nasolabial fold symmetry, and oral commissure symmetry with efforts at smiling, lip pursing, and frowning.
Hearing Test
Hearing loss is the most common complaint, with up to 80% of patients experiencing it. A 512 Hz tuning fork exam can distinguish a conductive hearing loss (CHL) from a sensorineural hearing loss (SNHL). An audiogram should be obtained 4–6 weeks following injury.
Radiological Evaluation
Computed tomography (CT) is the best modality for assessing temporal bone fractures ( Fig. 1.17.2 ). Opacification of air cells and pneumocephalus can suggest a fracture. Pneumolabyrinth suggests OC involvement and is found in up to 8% of fractures. A head, maxillofacial, or cervical CT can detect a fracture without the need for a dedicated temporal bone scan. The sensitivity and specificity of a maxillofacial CT scan in cases of blunt head trauma and associated vascular injury are greater than 90% and imply a negative predictive value of >95%. A separate HRCT can add cost, radiation exposure, and time to a work-up without significantly changing management. However, if standard imaging does not show a fracture but physical exam suggests its presence, or if management dictates the superior anatomical information offered by HRCT, then a dedicated temporal bone CT should be obtained. In cases where surgical management is considered or an unreliable clinical exam is present, a HRCT scan provides adjuvant information that changes treatment.


HRCT should include proper filters for bone edge detection and reconstructions from small fields of view with minimal slice thickness (e.g. 0.5 mm) and spacing (ideally 0 mm). Scans obtained with spiral technique or from multidetector scanners using 0.5 mm 3 or smaller voxels allow for reconstructions in any plane without loss of resolution. For pediatric patients, low-dose radiation protocols may be used; however, evaluation of small structures may be difficult. The evolution of flat panel CT is a promising development that may offer even higher resolution of bony anatomic detail with lower total radiation dose. No matter the technique used for HRCT, the clinician should review the images and correlate physical findings with imaging ( Box 1.17.1 ).
- •
Location and direction of temporal bone fracture
- •
Violation of otic capsule: cochlea, vestibule, semicircular canals, vestibular aqueduct
- •
Ossicular integrity: malleus, incus, stapes
- •
Facial nerve canal: internal auditory canal, fallopian canal, geniculate fossa, tympanic, mastoid
- •
Tegmen: tympani, mastoideum
- •
Vascular: carotid canal (petrous, cavernous), venous sinus (transverse, sigmoid, jugular bulb)
Fractures involving vascular structures should be examined with CT angiography as the stroke rate for carotid artery injury is 31%–33% in this population. Findings include vessel wall irregularity, changes in vessel caliber, abnormal outpouching, and occlusion of a vessel or a contrast blush indicating extravasation of blood. The gold standard is catheter angiography. In a retrospective review, 38% of patients with temporal bone fractures who underwent angiography had abnormal findings, including pseudoaneurysm, carotid dissection, and vasospasm.
Classification of Temporal Bone Fractures
Temporal bone fractures have traditionally been described as transverse, longitudinal, or mixed with respect to the petrous apex. Conceptually, transverse temporal bone fractures have fracture lines that run perpendicular to the long axis of the petrous bone, ending in the foramen magnum. Longitudinal fractures extend anteromedially to end generally in the foramen ovale or foramen lacerum. Roughly 80% of fractures are classified as longitudinal while 20% are transverse. CHL is more likely in longitudinal fractures while SNHL and facial nerve injuries are more likely in transverse fractures.
With the advent of HRCT, many fractures do not fit precisely into this classical pattern. Two alternative classifications have been proposed – OC sparing (OCS) versus OC violating (OCV) and petrous versus nonpetrous fractures.
OCV fractures involve the labyrinth and can present with SNHL, CSF otorrhea, and facial nerve paralysis. OCV fractures are 7–25 times more likely to develop SNHL, 4–8 times more likely to have a CSF leak, and 2–5 times more likely to develop facial paralysis.
Petrous fractures include OC as well facial nerve and carotid injuries. Nonpetrous fractures include injury to the mastoid (bone) and/or tympanic ring with potential damage to the ossicular chain and facial nerve.
Management, Surgical Indications, and Techniques
Temporal bone fractures rarely require surgical intervention. Exceptions exist for persistent CHL, facial nerve injury, CSF leaks with or without encephaloceles, and control of hemorrhage. In the acute period, otic drops help clear debris from the EAC. In a systematic review, Villalobos et al. found prophylactic antibiotics did not reduce the rate of meningitis in patients with skull base fractures.
Conductive Hearing Loss
CHL can occur in up to 58% of fractures, with an estimated 27% in the pediatric population. The most frequent cause of a CHL is hemotympanum. Treatment is observation, with the majority of patients improving to normal or near normal hearing levels. About 25% of CHL may persist beyond 6 weeks. The majority of traumatic TM perforations will heal within 3–5 months. In cases of persistent CHL without TM perforation or hearing loss greater than 30 dB, ossicular chain disruption should be considered. Ossicular abnormalities are found in 43% of patient with CHL, and the majority of ossicular pathology is related to the incus.
Hollinger et al. speculate that ossicular disruption is due to a transient deformation of tegmen tympani, pushing the incus inferiorly and tilting the stapes towards the promontory. Disarticulation of the incudostapedial joint and complete dislocation of the incus occurs. In cases of penetrating trauma, Hollinger et al. speculate the pressure wave created by a projectile causes a high frequency vibration within the chain leading to ossicular damage.
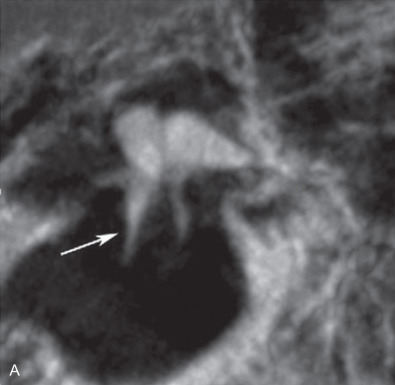
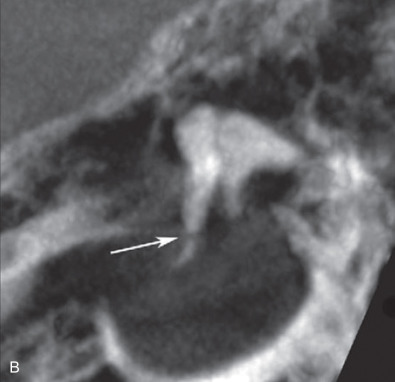
Ossicular fracture is more unusual. Tailored multiplanar reconstructions (MPRs) coupled with even higher-resolution techniques like flat-panel CT allow the neuroradiologist and otolaryngologist to visualize the entire ossicular chain to localize damage ( Fig. 1.17.3 ).
Middle ear exploration can be offered in cases of persistent CHL and if hearing is not severely impaired in the contralateral ear. The ideal time to explore is unknown. Early intervention may be premature; however, the longer one waits, the greater likelihood of ossicular chain fixation. Outcomes for surgical repair are good, with most patients improving by 20 dB to near or normal hearing levels.
Cranial Nerve Injury and Facial Nerve Paralysis
Cranial nerves VI, VII, VIII, and the lower cranial nerves including XII, can be injured in temporal bone trauma. Cranial nerve injuries can be difficult to assess due to life-threatening injuries and/or AMS. Almost 60% of deficits are documented greater than seven days after injury, with 15% identified more than a month later.
The facial nerve is the most commonly injured nerve, with a reported prevalence of 5%–54%. About 4% are bilateral injuries as a result of bilateral temporal bone fractures.
Contusion, edema, and hematoma of the nerve sheath are found in 86% of fractures with facial paralysis, while frank nerve section is rare. The ganglion and perigeniculate region is the most commonly injured site, followed by the vertical segment.
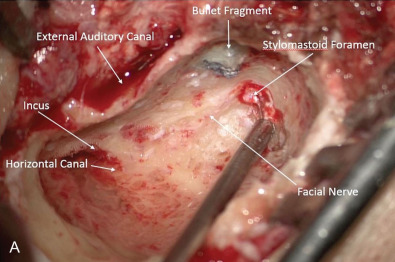
In GSWs, facial nerve injury rates have been reported to be between 15% up to 75%. Mechanical trauma and thermal injury can cause destruction to the nerve. The vertical segment and its exit at the stylomastoid foramen are common sites of injury ( Fig. 1.17.4 ).