| Suspicion of giant cell arteritis based on temporal headache, jaw claudication, scalp tenderness, weight loss or fever |
| Unexplained associated vision loss or pallid optic nerve edema; may be associated elevation of erythrocyte sedimentation rate (ESR) and/or C-reactive protein (CRP) |
| Visual acuity, pupillary reaction, visual field testing, color testing |
| Palpation of the temporal region for tenderness |
| Dilated funduscopic examination looking at optic nerve and retinal/choroidal vascular perfusion |
| History of prior scalp and facial surgery or trauma |
| History of rheumatologic conditions, including polymyalgia rheumatica |
| Laboratory studies, including ESR, CRP and complete blood count |
Introduction
The classic triad of giant cell arteritis (GCA) includes headache, scalp tenderness, and vision loss. The condition occurs as a result of granulomatous inflammation in the smaller to medium-sized vessels in the distribution of the external carotid, vertebral, ophthalmic, and posterior ciliary arteries. Additional constitutional symptoms may occur, consisting of jaw claudication, weight loss, malaise, and fevers. Patients are typically over 50 years of age and laboratory testing, including erythrocyte sedimentation rate (ESR), is particularly helpful in stratifying risk.
The oculofacial surgeon is frequently called upon to assist with diagnosis by performing the temporal artery biopsy. Patients with suspected GCA may be placed on prophylactic steroids prior to the biopsy; however, if the duration is longer than 2 weeks, this may interfere with the histopathological results. The temporal artery biopsy is typically performed unilaterally. If the first side is histopathologically negative, consideration should be given to performing biopsy of the contralateral side, as studies have shown that a small percentage of cases will be positive on the opposite side. For continued medical therapy after the biopsy, patients with GCA should be managed by a neuro-ophthalmologist and rheumatologist.
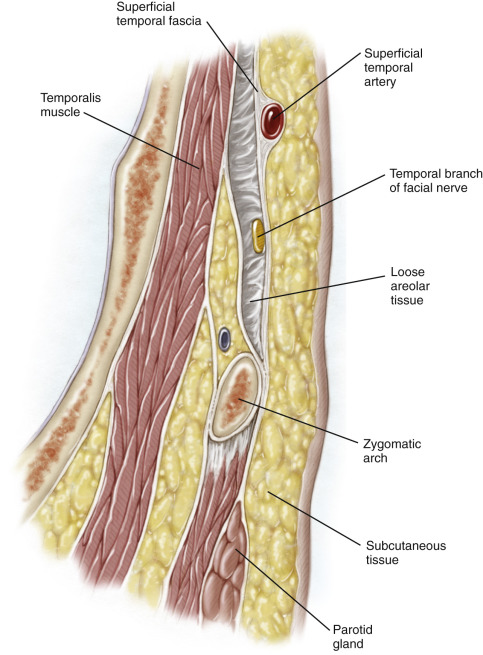
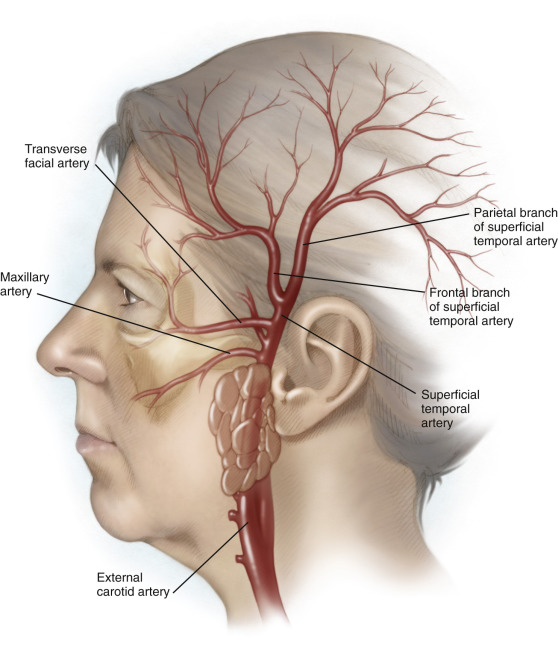
The superficial temporal artery (STA) is composed of two branches: the frontal branch and the parietal branch ( Figure 44.1 ). These vessels are terminal branches of the external carotid artery. The superficial temporal artery travels in the plane of the superficial temporal fascia (STF). This layer is just deep to the subcutaneous layer of the scalp and overlies the temporalis fascia proper. The frontal branch of the artery is typically the easiest to access for biopsy and is accessible through an incision made behind the hairline. The parietal branch may also be biopsied but this is often behind hair-bearing skin.
Preoperatively, the course of the artery should be palpated or traced with a Doppler flow detector if not palpable. The temporal branch of the facial nerve innervates the frontalis muscle and travels under the STF ( Figure 44.2 ). The course of the nerve is typically much more anterior and inferior to the course of the artery, as the nerve crosses the zygomatic arch at Pitanguy’s line, several centimeters anterior to the tragus. Approximately 2 cm superior to the lateral brow, the temporal branch of the facial nerve and frontal branch of the STA may potentially overlap. Dissection should be avoided in this area and, if necessary, the dissection should be kept within the plane of the STF to avoid damage to the nerve. If the dissection is kept closer to the hairline at the proximal root of the frontal branch of the STA, risk to the temporal nerve branch is minimal.