Techniques for Treating Nasal Airway Obstruction
Michael R. Lee
DEFINITION
Nasal airway obstruction (NAO) is a clinical diagnosis established through a focused history and physical examination. All patients undergoing rhinoplasty should be assessed for NAO.
The external nasal valve is located at the nostril. Nasal ala forms the lateral aspect of the valve, whereas the columella makes up the medial portion. Collectively, these structures with the soft triangle create the external valve.
The internal nasal valve is formed by the junction of the caudal portion of the upper lateral cartilage with the dorsal nasal septum.
Nasal septum is the anatomic structure that divides the nasal cavity. Made of bone and cartilage, the septum provides support for the nasal dorsum and tip.
Inferior turbinates are paired bones that extend medial into that nasal cavity from the lateral nasal wall. Turbinates regulate nasal airflow characteristics and provide mucociliary clearance.
ANATOMY
NAO typically occurs at one of four areas:
External nasal valves
Internal nasal valves
Nasal septum
Inferior turbinates
Understanding the anatomy of these structures is fundamental to treating NAO in rhinoplasty.
The external nasal valve relies on structural support of the lower lateral cartilages and adjacent soft tissue.
Lateral support is provided by fibrofatty tissue of the nasal ala and structural integrity of the lateral crura.
Medial support is provided by the caudal septum, medial crura, and soft tissue of the columella.1
The term basal aesthetic lines (BALs) is used to describe this lateral border of the columella. BALs should exhibit a smooth slightly concave slope with no protrusion into the nostril (FIG 1A).
Each upper lateral cartilage is supported cephalically by the nasal bone, laterally by the frontal process of the maxilla, and medially by the dorsal nasal septum.
As form and function are closely related in rhinoplasty, structurally sound middle nose anatomy is usually associated with ideal dorsal aesthetic lines (DALs).2
Confluence of the caudal upper lateral cartilage and dorsal nasal septum is most often a site of NAO as it forms the internal nasal valve.
The internal nasal valve is the area of greatest restriction in terms of nasal airflow (FIG 1B).
The nasal septum provides crucial support for the external nose.
Seated firmly on the maxillary nasal spine, the septum provides support for the overlying upper and lower lateral nasal cartilages.
The dorsal septum is responsible for creation of the internal nasal valve.
The caudal septum extends beyond the maxillary nasal spine and provides structural support for the medial nasal base.
It is flanked by medial crura and intimately related to soft tissue structures of the columella.1
The inferior turbinate extends from the lateral nasal wall into the lower nasal cavity.
Its proximity to the internal nasal valve makes hypertrophy problematic when present.
Although turbinate architecture is primarily a function of the bone, the overlying erectile tissue and surface mucosa contribute greatly to nasal function.
Erectile tissue fluctuates, thereby altering nasal resistance, and directly influences nasal airflow.
The respiratory mucosa provides immunologic benefit and mucociliary clearance.
DIFFERENTIAL DIAGNOSIS
Stenosis/collapse of the external nasal valve
Stenosis/collapse of the internal nasal valve
Septal deviation
Septal spur formation
Inferior turbinate hypertrophy
Nasal mass or polyp
PATHOGENESIS
Intranasal deformity may result from congenital development, traumatic injury, or iatrogenic insult. Changes in nasal support and physiology may occur with aging resulting in NAO.
Traumatic injury to the nasal septum may be classified by fracture patterns.3
High-impact trauma is associated with multiple septal fractures and displacement from the maxillary nasal spine.
PATIENT HISTORY AND PHYSICAL FINDINGS
Relevant history in the obstructed patient includes laterality, timing and duration, worsening or alleviating factors, perennial or seasonal response, prior nasal surgery or trauma, and associated symptoms.
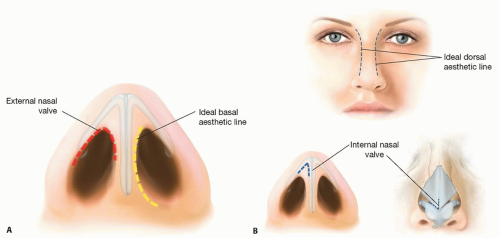
FIG 1 • A. Diagram of the external nasal valve. Nasal ala constitutes the lateral valve, whereas the columella creates the medial aspect. Note the ideal basal aesthetic line. B. Diagram of the internal nasal valve. Amalgamation of the caudal edge of the upper lateral cartilage to the dorsal septum creates the valve. Note the ideal dorsal aesthetic line.
Progressively worsening symptoms and associated epistaxis should raise concern for neoplasm.
Inspection of the nasal airway begins with study of the nasal base at rest and during respiration.
The external valve is assessed initially.
Inspection should reveal a patent nostril, free of obstruction.
At rest, the lateral nostril (nasal ala) should demonstrate a stable, convex architecture.
The medial nostril (lateral columella) should exhibit ideal BALs.
External valve stenosis may be the result of obstruction from either of these directions.
Assessment during respiration is also performed to determine if collapse of the external valve is responsible for symptoms.
Inspection of the internal nasal valve is accomplished with a nasal speculum. Care must be used to avoid widening of the valve on speculum insertion.
The upper lateral cartilage caudal margin can be readily appreciated through the nasal mucosa.
The angle created by the junction of this caudal margin and the dorsal septum is assessed.
A narrow angle at baseline suggests stenosis of the valve.
Collapse of the internal valve on respiration may also be identified as a cause for NAO. The Cottle test can confirm internal valve insufficiency.
Evaluation of the septum also begins at the nasal base.
Deviation of the caudal septum to either side can obstruct the external valve.
Palpation and manipulation of the columella will clearly identify caudal septum position.
Examining the dorsal septum and septal body is performed with nasal speculum.
Deviation of the dorsal septum is determined as this may cause stenosis of the internal nasal valve.
The body of the nasal septum is surveyed for deviation and spur formation, either of which may cause NAO.
The inferior turbinate is next examined also with use of a speculum.
Turbinate size, position, and tissue characteristics should be noted.
A large, boggy inferior turbinate with a bluish hue is associated with allergic response. These patients will likely have some degree of refractory symptom despite surgical reduction.
The location of turbinate hypertrophy guides surgical reduction and should be noted.
Topical oxymetazoline is applied to determine the response to medical decongestant.
If topical treatment results in symptom resolution, a medical management trial is warranted. This often includes topical steroids and routine nasal toilet.
Intranasal examination should also rule out less common etiologies of nasal obstruction such as nasal polyps and neoplasms.
IMAGING
Although plain radiographs and computed topography can be used to evaluate nasal septum and turbinate position, they are not routinely required. NAO is a clinical diagnosis that results primarily from a focused history and physical examination.
If concerns arise of other NAO causes, such as neoplasms or polyps, proper consultation and imaging are warranted.
NONOPERATIVE MANAGEMENT
Patients who display any suggestion of an allergic component to their NAO should undergo a medical trial.Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Technique for Ptosis Correction
Technique for Ptosis Correction
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Indications and Techniques for Short-Scar Face-Lift
Indications and Techniques for Short-Scar Face-Lift
 Technique for Ethnic Rhinoplasty Using the Open Approach
Technique for Ethnic Rhinoplasty Using the Open Approach
 Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


