Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Ashkan Ghavami
DEFINITION
Augmentation of the nasal bridge and radix has historically been a highly debated topic in rhinoplasty.
Techniques include alloplastic materials such as silicone implants, Gore-Tex, and PTFE. Although these techniques continue to be popular worldwide, particularly in Asian countries, there has been a paradigm shift toward autogenous sources. Preferred cartilage grafts include septal, costal, and conchal cartilage. Each of these in isolation is fraught with problems in stability of shape and long-term contour.
Erol’s description of the “Turkish Delight,” which is diced cartilage wrapped in Surgicel, provided a simple, less complicated option for dorsal augmentation.1 Not long after, Daniel2,3 described wrapping with autogenous temporal fascia (DCFG: diced cartilage fascia graft) as an alternative; this has become many surgeons’ primary technique today. It should be noted that temporoparietal grafting to the nose in isolation was described long ago by Guerrerosantos in 1985.4
The author’s preferred material is conchal cartilage, but costal cartilage and/or septal remnants can be used.
Fascial wrapping and/or overlay of the cartilage construct allows for incorporation of the graft and smooth contour in surgical outcomes. Contour irregularities from warping with other autogenous techniques have been a long-standing problem that is avoided with DCFG when properly executed.
This technique can be particularly useful in secondary rhinoplasty.2
ANATOMY
Anatomical landmarks and technical execution of harvesting the cartilage grafts to be diced/crushed are imperative to avoid injury or deformation of donor sites at the expense of obtaining cartilage source.
Standard techniques for harvest of rib, septal, and conchal elements can be used based on the surgeon’s personal preference.
For conchal grafts, a postauricular approach is performed. Rib graft typically is taken from the sixth or seventh rib, and it is important to not harvest calcified portions that are difficult to dice and/or morselize sufficiently. The inframammary crease is used in both men and women.
Temporal, mastoid, and rectus fascia can all be used.
Goals are based on the desired contour and degree of augmentation/camouflaging required. This begins at the radix and proceeds caudally to the supratip and anterior septal angle region.
Blending with the osteotomy lines and the ascending process of the maxilla as it transitions to the nasal bones is important to create a smooth nasal sidewall contour and soft contour shadow/highlight.
“Spot” augmentation with DCFG can be done in radix alone or to fill specific contour irregularities (particularly in secondary revision cases).
PATIENT HISTORY AND PHYSICAL FINDINGS
Particularly in the modern era of social media and a “selfieobsessed” culture, it is absolutely critical to communicate the magnitude of augmentation desired by the patient while setting realistic expectations.
Accounting for the somewhat unpredictable long-term absorption rates is also important to communicate with the patient.
The author believes that the trade-off of minor to moderate long-term absorbability of DCFG for complications associated with traditional augmentation techniques (warping, extrusion, unnatural dorsal contour lines, need for removal, and replacement/reconstruction) is highly acceptable in favor of DCFG.
After the standard workup for rhinoplasty with imaging and planning, desired dorsal contour is obtained during the consultation. Attention is given to the width and height of desired dorsal augmentation. If specific camouflaging or contour correction is planned, then these regions should be pointed out to the patient with the end points described or shown via imaging, drawings, or demonstration with saline (in-office).
IMAGING
Three-dimensional imaging software as well as 2D imaging or drawings are helpful in communicating the amount of dorsal height and narrowing/widening with patients.
The author currently prefers to demonstrate with description and reference to other surgical case examples during consultation. Hand drawings on printed out photographs are helpful, and only when necessary during repeat consultation(s) or during the preoperative office visit is 3D imaging utilized.
X-rays or CT scans are not necessary unless there is history of recent or remote trauma or if concomitant nasal airway correction or sinus surgery is planned.
When costal cartilage is used, assessment of possible excess calcification of the ribs should be done. This can include needle testing in the exam room using minimal local anesthesia and/or CT scan evaluation when truly necessary.
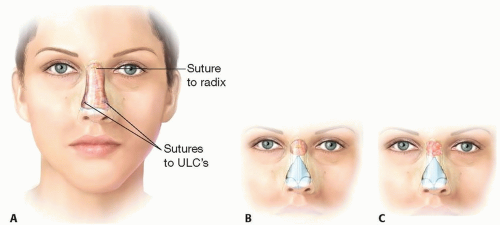 FIG 1 • A. Anteroposterior view of proper DCFG positioning on dorsum. B. Variation: radix-only DCFG. C. Variation: radix-only DCG. No fascia necessary due to thick nasal skin. |
NONOPERATIVE MANAGEMENT
There is no substitution for DCFG that is nonoperative and long term that is justified in the author’s opinion. However, as an adjunct to planning and only when a patient is not ready for surgery for a year or more, temporary injectable fillers can be a useful tool and “buys time.” Hyaluronic acid gel fillers are preferred, and any other filler material is not recommended.
A major limitation of nonsurgical filler augmentation is that dorsal aesthetic lines in the anteroposterior view are difficult to optimize because narrowing of the nasal pyramid is not being simultaneously performed.
The one region that may warrant dorsal augmentation with temporary fillers instead of DCFG is in the radix when all other aspects of the nasal shape are accepted by the patient. Consultation should include surgical options and informed consent of the temporary nature of injectable fillers for the radix or for minor contour correction.
One of the best indications for injectable (nonoperative) dorsal augmentation is for minor/subtle contour correction of dorsal and other irregularities (primary and secondary rhinoplasty). Small molecule, highly cross-linked hyaluronic acid gel is best and must be injected with respect of vascular dermal capacitance.
SURGICAL MANAGEMENT
Preoperative Planning
Planning DCFG augmentation in rhinoplasty involves many of the methods listed above:
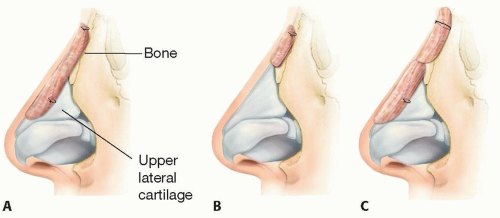
FIG 2 • A. Lateral view of typical DCFG seating and suturing for dorsal augmentation. B. Lateral view showing DCFG for radixonly augmentation. C. Lateral view: variation of using two DCFG constructs. Note: Cephalad fixation is done performed using sutures through the dorsal skin. Caudal DCFG is to cartilages.
Detailed consultation with the patient with regard to the desired goals in dorsal augmentation is paramount. This includes dorsal height, dorsal aesthetic contour width, and supratip/other tip transition points to the dorsum.
Imaging as discussed above can aid in this process.
Saline solution can be injected in the office to show an approximate effect of dorsal augmentation on profile view if the surgeon and patient agree that this step is necessary to finalize the decision-making process.
Standard rhinoplasty preoperative planning is performed including attention to internal and external valve sufficiency, airway assessment, Cottle maneuver, nasal endoscopy (when indicated), and evaluation of cartilage donor sites.
Note: augmentation of the dorsal height and/or narrowing of the bony pyramid and midvault can worsen airway functional issues. Dorsal height augmentation can mask these issues visually, while untreating the underlying insufficiency and patency of the airway. Dorsal width changes with DCFG must be reconciled with the need for spreader graft/flap techniques.
DCFG is not a substitute for proper osteotomies and correction of sidewall irregularities and asymmetries. The platform for the DCFG construct must be stable, symmetric, and structurally sound prior to using DCGF for augmentation and/or contouring.
Marking of the topographical dimensions can be done both on the patient in the holding area on day of surgery and on photographs.
Donor sites:
Ear: The preferred sleeping side is avoided, and the contralateral ear is used when possible. Concomitant correction of prominent ears allows for more graft material, and discussion with the patient is indicated. If the patient has a small conchal area, then the larger concha is used, or bilateral conchal graft is planned.
Rib: The inframammary crease is marked in both men and women, and the rib is accessed through the smallest incision the surgeon is comfortable with. This is typically the sixth or seventh rib. Incision placement should be shown to the patient preoperatively.
Fascia: The temporal, mastoid, or rectal fasciae are all options. When using costal graft, the author prefers rectus fascia because it is thick and in the same donor site. When this would be too thick and not indicated for a particular nasal envelope, temporal fascia is then harvested. When using ear cartilage, mastoid fascia is taken. If mastoid fascia is not large enough and true wrapping is required, then ipsilateral temporal fascia is obtained through a prehairline approach.
Positioning
Standard head positioning for rhinoplasty is used with the patient in the supine position and the head of bed in reverse-Trendelenburg, as well as head elevation, approximating a 30 to 45 degree angle.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree