Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Oren M. Tepper
Jillian Schreiber
Elizabeth B. Jelks
Glenn W. Jelks
DEFINITION
The periorbital region is an essential component of a youthful appearing face. Aesthetic rejuvenation of the eyelids is a frequently requested and challenging procedure offered by most plastic surgery practices. Although soft tissue descent and cutaneous changes have long been recognized as a sign of periorbital aging, volume loss or deflation has more recently been appreciated as an important contributing factor as well.1,2
Traditional blepharoplasty is subtractive in nature. Conventional approaches to upper and lower blepharoplasty include excision of excess skin and fat, with potential risk of creating a hollowed or “operated” appearance.2,3,4 In light of the importance of periorbital fat to provide support and contour in the youthful eyelid, there has been a shift in blepharoplasty techniques away from excision alone toward preservation and restoration of periorbital volume.2,5,6,7 The goals of this chapter are to provide an updated approach to fat grafting in the periorbital region as a primary means of achieving upper and lower eyelid rejuvenation and/or correction of secondary deformities.
Autologous fat grafting has gained widespread popularity as an effective means of volume augmentation for various facial procedures due to its ease of harvest, longevity, rapid execution, and relative safety.8,9,10 Autologous fat grafting is used to address changes due to aging in the upper and lower eyelid, the brow, and the eyelid-cheek junction.1
Upper Eyelid
Atrophy of fat and skin in the upper eyelid and surrounding regions can result in skeletonization of the bony orbit, protuberance of remaining periorbital fat, poor soft tissue support, and eyebrow descent.
In general, fat grafting of the upper eyelid is most commonly performed for correction of a hollowed appearance to the upper eyelid sulcus. This may be the result from aging or secondary to over-resection of retroseptal fat during an upper blepharoplasty procedure.
Lower Eyelid
A prominent nasojugal groove, often described as the “tear trough,” is a common finding in patients seeking periorbital rejuvenation. The anatomical junction of the lower eyelid and cheek (palpebral malar interface) extends from the medial canthus inferolaterally above cheek tissue to form a depression (nasojugal groove). This is distinct from colloquial terms such as “dark circles” and “puffiness” of the lower eyelid that are commonly used interchangeably.
Fat grafting to the eyelid-cheek junction, with or without skin and fat excision, is an effective means to treat a tear trough deformity and camouflage the prominence of fat in the lower eyelid compartments.
ANATOMY
The periorbital region is composed of the bony orbital rim, orbicularis oculi muscle, orbital fat compartments, and the upper and lower eyelids. The upper and lower eyelids are layered structures composed of an anterior and posterior lamella divided by the orbital septum (FIG 1).
The thin eyelid skin and orbicularis oculi muscle constitute the anterior lamella of the upper and lower eyelids. The orbicularis oculi muscle is divided into pretarsal, preseptal, and orbital components. The pretarsal and preseptal portions make up the palpebral segment and provide involuntary blink, whereas the orbital portion provides voluntary eyelid closing.
The posterior lamella is composed of different but analogous structures between the upper and lower eyelids. The upper eyelid posterior lamella includes the palpebral conjunctiva and tarsal plate. Above the tarsal plate, it is composed of the palpebral conjunctiva and Müller muscle. The posterior lamella of the lower eyelid is similarly made up of the palpebral conjunctiva and tarsal plate and inferior to the tarsal plate the conjunctiva and capsulopalpebral fascia and inferior tarsal muscle.
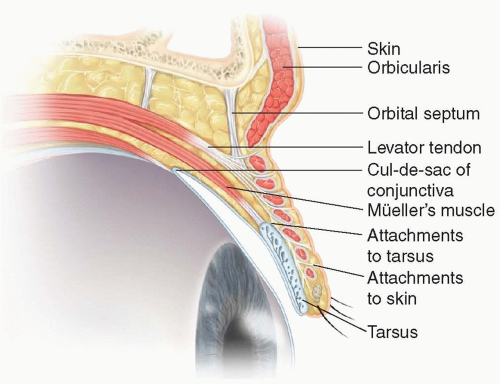
FIG 1 • Upper eyelid anatomy. Sagittal section through the upper eyelid demonstrating the anterior and posterior lamella and the relationship with the orbital septum.
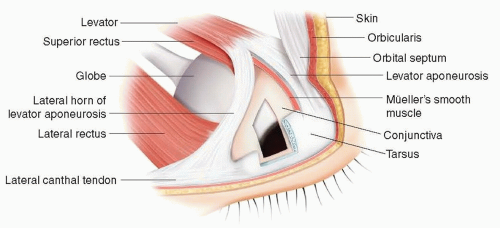
FIG 2 • Upper eyelid anatomy highlighting the relationship between the levator muscle, the tarsus, and lateral canthal tendon.
The upper eyelid retractors are the levator palpebrae superioris innervated by the oculomotor nerve and the sympathetically innervated Müller muscle (FIG 2). The lower eyelid retractors include the capsulopalpebral fascia and inferior tarsal muscle.

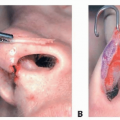
FIG 3 • Periorbital fat compartments of the lower eyelid and cheek. A. The medial suborbicularis oculi fat compartment (MSOOF). B. The deep medial cheek fat compartment. C. Addition of the MSOOF, DMC, and the lateral suborbicularis oculi fat compartment (LSOOF).
The prominent tear trough is often addressed in periorbital rejuvenation. Factors that contribute to a prominent palpebral malar interface include alterations in the quality and elasticity of the overlying skin, subcutaneous tissue, orbicularis oculi muscle, orbital septum, capsulopalpebral fascia, and retroseptal orbital fat.2 The anatomical position of the arcus marginalis on the zygomatic and maxillary bones determines the location of the palpebral malar interface2,3 (FIG 4).
The arcus marginalis is defined by the bony origin of the orbital septum, orbital periosteum, and the maxillary periosteum. The origins of the preseptal and orbital orbicularis oculi muscle, the orbital retaining ligaments, malar septum, prezygomatic space, and arcuate bands are related to the arcus marginalis.
The upper eyelid fat is composed of the medial and lateral fat compartments. In the lower eyelid, three distinct fat compartments of retroseptal fat exist: lateral, central, and nasal. The nasal and central compartments are divided by the inferior oblique muscle tendon. The medial (nasal)
compartment is derived from the white orbital fat and the lateral (central) fat compartment from the less dense, yellow preaponeurotic fat.1
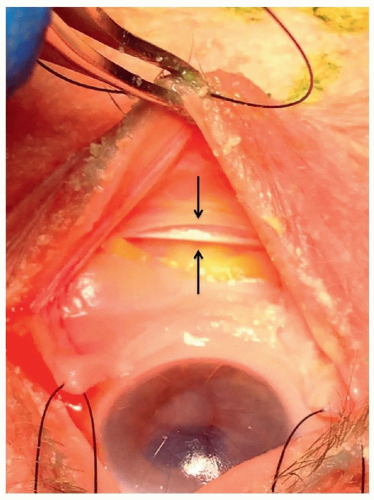
FIG 4 • The arcus marginalis is shown on cadaveric dissection. It is the bony origin of the orbital septum, orbital periosteum, and the maxillary periosteum.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access