Technique for Treating the Long Nose
Michael R. Lee
Rod J. Rohrich
DEFINITION
Long nose is a term used to describe a nose that extends beyond the ideal nasal length. Multiple subsites may be responsible for creating a long nose and will be discussed.
Nasal length is measured from the root of the nose to the most projected part of the nasal tip. Ideally, nasal length should measure 0.67 of the midfacial height (eyebrow to subnasale).
Nasal projection is measured from the alar groove to the most projected part of the nasal tip. Ideally, nasal projection should measure 0.67 of the ideal nasal length.1
Nasal rotation is determined by using the nasolabial angle. On lateral view, a line is drawn bisecting the long axis of the nostril, whereas a second vertical line is drawn through the anterior most aspect of the upper lip. The angle created should fall between 90 and 110 degrees in women and between 90 and 95 degrees in men. A more obtuse angle is associated with over-rotation of the tip, whereas a more acute angle is associated with a decreased tip rotation. The latter is often seen with the long nose.
ANATOMY
Increased nasal length may result from multiple anatomic subsites including the radix and nasal bones, dorsal and caudal nasal septum, and/or excess paired nasal cartilages. These structures may be solely responsible for the long nose, but more often it is a combination of subsites (FIG 1).
The nasal skin and musculature envelop the underlying bone and cartilage. Soft tissue attachments work to keep proper relationships between nasal bone and cartilage. These attachments provide support for the nasal tip.
Nasal tip support structures can be divided into major and minor. Major tip support structures include the fibrous attachments between the upper and lower lateral cartilages (scroll ligament), lateral crura and pyriform aperture, medial crura and caudal septum, and the interdomal tip ligament. Minor tip support structures include fibrous attachments of alar cartilage to the cartilaginous dorsum, alar cartilage attachments to overlying skin, and the membranous septum.1
PATHOGENESIS
A long nose may occur as the result of congenital development, traumatic injury, iatrogenic injury, and/or aging.2,3 Congenital overgrowth may lead to volume excess. Traumatic injury may displace or activate growth of bone or cartilage. Iatrogenic injury may create a long nose when tip support is not properly established. Aging results in loss of tip projection and midface volume loss, both of which contribute to a long nose.
The illusion of a long nose may occur in patients with subnasale malposition, periapical hypoplasia, short midface, or inadequate chin projection.
A true increase in nasal length may occur with a high radix, excess volume of the upper lateral cartilages, lower lateral cartilages, nasal septum, and/or loss of tip projection.
PATIENT HISTORY AND PHYSICAL FINDINGS
Aesthetically, patients may feel their nose is simply too large for their face. As the focal point of the face, a long nose often disrupts nasofacial balance.
Patients may point out a large hump caused by excess bony or cartilaginous dorsum. They may complain of a prominent or hanging columella that results from excess of the caudal septum. Patients may also report a drooping tip from inadequate support.
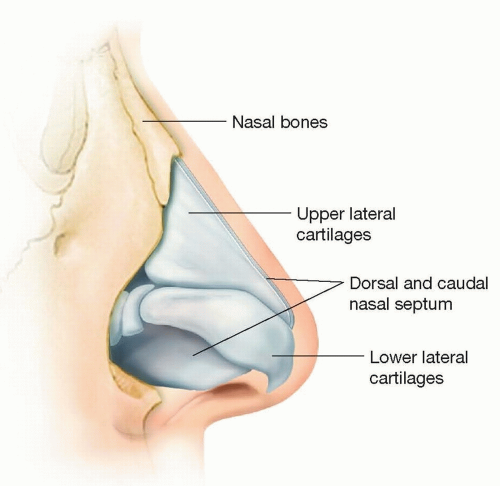
FIG 1 • Illustration depicting the nasal substructure. Increased nasal length may result from multiple anatomic subsites including the radix and nasal bones, dorsal and caudal nasal septum, and/or excess paired nasal cartilages.
Examination begins with assessment of facial widths and vertical heights. This is important as the overall surgical goal is to create improved balance between the face and nose. If the facial proportions grossly deviate from aesthetic ideals, this is taken into consideration when creating the operative plan.
The nose is evaluated in all classic rhinoplasty views with attention focused on areas responsible for creating a long nose. The patient is examined in repose, animation, and respiration as the nose is a dynamic structure.
Anterior inspection is useful to determine symmetry and straightness, both of which contribute to the dorsal aesthetic lines (DALs). A large dorsal hump may distort the DALs.
Tip definition and position are also noted.
Lateral and oblique views are useful in the long nose. Evaluation begins with critique of the radix or nasal root. A high radix may be responsible for creating a long nose, whereas a low radix may give the nose an overprojected appearance. Next, the dorsum is inspected for the presence of a convexity (hump) or irregularities. Overgrowth of the upper lateral cartilages and/or dorsal septum is typically responsible for dorsal convexity. Distally, overgrowth of the caudal septum can downwardly displace the lower lateral cartilages. Overgrowth of the lower lateral cartilages can further contribute to caudal tip position. Caudal septal excess may also distort the alar-columellar relationship and create excess columella show.
Basal view analysis provides additional information in the long nose patient. Excess lower lateral cartilage volume may create domal fullness and disrupt the ideal columellar:tip ratio of 2:1. The basal aesthetic lines (BALs)4 are studied as they may be distorted by excess lower lateral cartilage volume and malposition of the medial crura.
IMAGING
3D imaging is extremely helpful in the long nose and improves communication between the surgeon and patient. Modern-day imaging software can readily display the anticipated changes of hump reduction, increased nasal rotation, and decreased nasal projection.
Imaging can also be useful to illustrate to patients the difference chin surgery or midface volume restoration can make in overall nasofacial harmony.
SURGICAL MANAGEMENT
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


