Technique for Ethnic Rhinoplasty Using the Open Approach
Dean M. Toriumi
Jeffrey T. Steitz
DEFINITION
The ethnic nose is very diverse and can encompass many different nasal contours and anatomic variations. It is outside the scope of this chapter to cover all of these anatomic variations. For this chapter, I will cover the Black and Asian nose and how I use the open approach to perform structural grafting to augment the nose.
When I use the term “ethnic” in this chapter, I will be referring to primarily Black and Asian patients. These techniques may also prove to be effective in the thick-skinned “Mestizo” nose. This is with the understanding that there are many other forms of ethnic noses that have significantly different anatomy but will not be emphasized in this chapter.
Many ethnic patients have an underprojected nose with a wide alar base and poorly defined nasal tip. These patients also tend to have thicker skin. They can have a low wide dorsum lacking definition on frontal view. Some ethnic patients may have a dorsal hump with a low radix. All of these different configurations require different management.
In general, most Black and Asian patients require augmenting their nose to stretch the thick skin envelope to create improved contour. This requires cartilage grafting to push out and stretch the thick skin envelope making the lateral view larger to enhance the appearance of the frontal view.
ANATOMY
The anatomy of the Black and Asian nose can vary significantly from patient to patient. Most ethnic patients will tend to have thicker sebaceous skin that is much thicker in the lower half of the nose. They tend to have weak lower lateral cartilages that can make controlling and preserving tip projection very difficult.
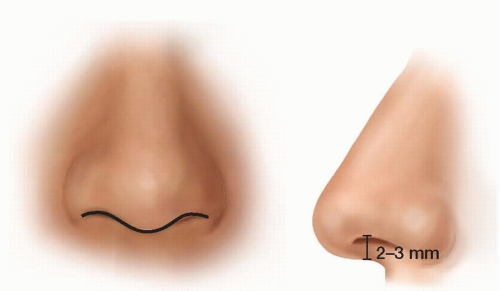
FIG 1 • The normal relationship between the infratip lobule and ala demonstrates a “gull in flight” appearance on the frontal view. This translates to a 2- to 3-mm columellar show on the lateral view.
Ethnic patients tend to have a short weak nasal septum that lacks caudal projection leaving a deficiency in tip support. For this reason, adding structural support is critical to providing a good aesthetic and functional outcome.
Ethnic patients may demonstrate a reversal of the normal “gull in flight” appearance of the transition from alar margin to infratip lobule (FIG 1).1 Many of these patients will demonstrate a reversal of normal with retraction of the columella in relation to the hanging alar lobule (FIG 2). Correction of the retracted columella requires a large caudal septal extension graft that can push the columella and infratip lobule inferiorly to create a more normal “gull in flight” appearance to the alar lobular transition to the infratip lobular projection.2 This graft will act to move the columella/infratip lobule or central compartment inferiorly to create a more favorable relationship between the ala and infratip lobule.
Ethnic patients also tend to have a wide alar base that creates a discrepancy between the width of the upper third of the nose and the width of the lower third of the nose. It is preferable to avoid overnarrowing the upper third of the nose with aggressive lateral osteotomies to create narrowing and then accentuate the imbalance between the upper third and lower third widths.
PATIENT HISTORY AND PHYSICAL FINDINGS
The patient should be examined to assess nasal tip support and caudal projection of the septum.
Intranasal examination should be performed using a nasal speculum, appropriate lighting, and preferably examination
with an endoscope. Assess the nasal septum and status of the inferior turbinates. Watch the patient breathe in to determine if there is any lateral wall weakness, which is rare in Black and Asian patients.
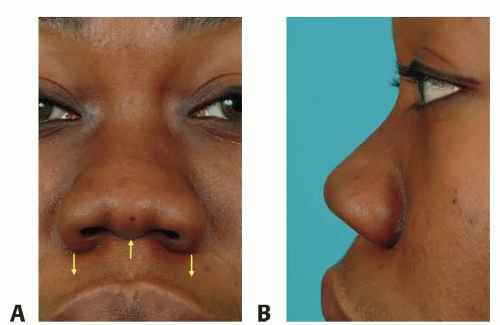
FIG 2 • A Black patient with retracted columella and hanging ala to create the opposite of the normal “gull in flight” orientation between the infratip lobule and ala. A. Frontal view showing the ala projecting inferiorly to greater extent than the columella/infratip lobule. B. Lateral view showing hidden columella.
Discuss with the patient what the primary goal of the surgery should be. Determine their primary deformities they would like corrected.
The deficiency in nasal tip support and reversal of the normal “gull in flight” orientation of the ala and columella must be pointed out to the patient.
Preoperative computer imaging is critical in the ethnic patient and should be used in most patients. This will enhance your ability as the surgeon to determine what the patient’s goals are and to point out specific concepts to the patient. This will help ensure your aesthetic goals align with those of the patient.
The linkage between lack of structural support and the large thick skin envelope must be pointed out to the patient as well.
One of the key concepts in ethnic rhinoplasty (Black and Asian) is to realize that it is usually necessary to augment the lateral view via dorsal augmentation, place a caudal septal extension graft and possibly a shield-type tip graft to stretch the thick skin, and create a narrowing effect on the lateral view. By stretching the skin on the nose, particularly in the nasal tip area, definition can be increased and narrowing can be achieved. This can be very difficult for both the surgeon and patient to understand, but thick-skinned patients rarely look better when the nose is reduced unless the skin is able to contract. Typically, the thicker skin of the lower third of the nose will not contract significantly, potentially leaving a polly beak deformity, a wider scarred nasal tip, and an underprojected tip complex.
Expanding and augmenting the lateral view can also improve the lateral view by lifting the upper nasal dorsum to match the projection of the prominent thicker supratip skin by creating a straighter profile (FIG 3).
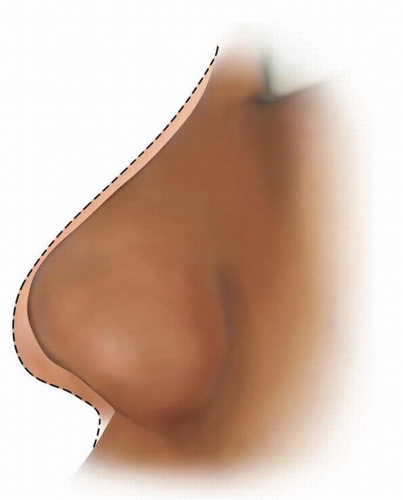 FIG 3 • By augmenting the lateral view, the upper nasal dorsum can frequently be elevated to the level of the prominent supratip skin creating a straighter dorsal line. |
SURGICAL MANAGEMENT
It is preferable to perform these surgeries under general anesthesia. With the patient intubated, the airway is protected from blood contacting the vocal cords and potentially causing laryngospasm. A protected airway is particularly important if any work is planned on the nasal septum or turbinates.
Local anesthetic agent (1% lidocaine with 1:100 000 epinephrine) is injected into the nose to provide hemostasis. Injections are made along the septum, along the marginal incisions, over the nasal dorsum and middle vault, and in the nasal tip area. At least 10 minutes should pass before the procedure is initiated to allow the full vasoconstrictive effect to set in.
TECHNIQUES
▪ Harvesting Cartilage for Grafting
Auricular cartilage can be harvested but is not ideal for grafting. The auricular cartilage is softer and weaker than costal cartilage and usually not adequate for augmentation cases. If auricular cartilage is harvested, the posterior approach is preferred to minimize the chance of ear deformity or change in position.
In most ethnic patients, a larger amount of cartilage is needed for grafting. Costal cartilage is preferable and can be harvested from a smaller 11-mm incision3 (TECH FIG 1A). It is recommended to use a larger incision when less experienced because safety is most important when harvesting costal cartilage.
The 6th or 7th ribs are ideal for cartilage grafting material in the ethnic patient. If a longer dorsal graft is needed, it is preferable to use the seventh rib as it is straighter and longer. The 6th rib tends to have a genu that will shorten the straight segment that could be used for dorsal augmentation. If both dorsal augmentation and premaxillary augmentation need be performed, two costal cartilage grafts may be harvested.
Costal perichondrium should be harvested as well, because this material can be used for camouflage and to aid in fixation of the dorsal graft to the underlying dorsal nasal bone. In these cases, the costal perichondrium is
placed as an interpositional graft that is sutured to the undersurface of the dorsal graft. The nasal dorsum is rasped or perforated with a 3-mm straight osteotome, and then the dorsal graft with perichondrium is placed over the nasal dorsum. The perichondrium will rigidly fix the dorsal graft to the underlying nasal dorsum.
 TECH FIG 1 • A 4.5-cm segment of costal cartilage harvested through an 11-mm incision. |
▪ Open Approach
An inverted-V incision is made at the level of the midcolumella (TECH FIG 2A). The position of the incision can be varied depending on the goals of the surgery. In most ethnic patients, the goal is to increase nasal tip projection.
The columellar incision is connected to bilateral marginal incisions made along the caudal margin of the lateral crura.
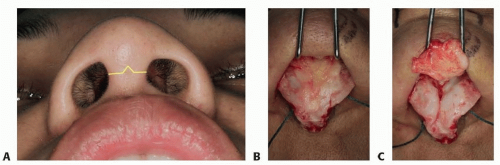
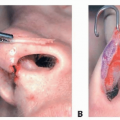
TECH FIG 2 • A. Position of the inverted-V midcolumellar incision marked out in yellow. B. A Black patient with thick skin after flap elevated leaving fibrofatty tissue on the lower lateral cartilages. C. After fibrofatty tissue dissected from cartilages.
The columellar flap is elevated off of the medial crura. Care is taken to avoid damaging the columellar flap.
During flap elevation, dissection can be performed just below the subdermal plexus leaving the fibrofatty tissue of the nasal tip and supratip on the cartilages to then be excised (TECH FIG 2B,C).
▪ Exposing the Nasal Septum
Dissection is performed between the medial crura to access the caudal septum. Typically, the caudal septum is further cranial than in most Caucasian patients (TECH FIG 3). After identifying the caudal septum, mucoperichondrial flaps are elevated.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree