Techniques for Placing Malar Implants
Erez Dayan
Dev Vibhakar
Michael J. Yaremchuk
DEFINITION
Prominent malar bones are considered attractive and youthful in most cultures.
The malar area is a dynamic anatomic region of the face composed of underlying skeletal support, adipose tissue, and mimetic muscles of facial expression.1
Characterization of the domelike shape of the malar area is largely subjective due to the lack of anthropometric and cephalometric landmarks. The inability to define “average” or “normal” for the malar area makes selection of implant shape, size, and position challenging.
ANATOMY
Skeleton
The malar eminence is the most projecting portion of the zygoma. Its convexity extends from lateral to the infraorbital foramen to the midaspect of the zygomatic arch.
It is perforated in its midaspect by the zygomaticofacial foramen for the passage of the zygomaticofacial nerve and vessels.
Muscles
Muscles of the midface largely provide facial expression. Those that are freed from their origins during malar augmentation elevate the upper lip and include zygomaticus major, zygomaticus minor, levator labii superioris, and levator anguli oris (FIG 1).
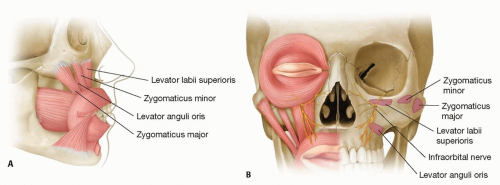
FIG 1 • A,B. Relevant facial musculature and intraorbital nerve in relation to malar implant placement.
Nerves
The infraorbital nerve exits the maxilla through the infraorbital foramen and travels beneath the levator superioris and above the levator anguli oris. Its branches supply the skin of the lower lid, the side of the nose, most of the cheek, and the upper lip. This nerve must be identified and preserved.
The zygomaticofacial nerve exists through a small foramen located on the lateral aspect of the malar bone. It supplies a small portion of the skin of the upper cheek. It is routinely sacrificed during malar augmentation.
PATHOGENESIS
Most frequently, patients who present for malar augmentation are within normal range and desire more definition, angularity, or balance to their facial contour.
Studies have demonstrated retrusion of the midface and mandibular skeleton with aging, thus supporting alloplastic augmentation of the skeleton as a component of the facial rejuvenation armamentarium.
Malar deficiency is often part of a generalized midface deficiency requiring soft tissue evaluation and treatment. As aging occurs, the retaining ligaments of the midface attenuate and soft tissues atrophy, leading to deflation and descent of the malar soft tissue complex.3,4
Functionally, malar projection provides a platform to support overlaying the soft tissue as well as provide some protection against lower lid descent (FIG 2).
Patients with craniofacial deformities often have functional and aesthetic consequences requiring more invasive
osteotomy and skeletal repositioning rather than malar alloplastic augmentation. However, in skeletally deficient patients with normal occlusion, alloplastic augmentation is often a more appealing option due to its less invasive surgery.5
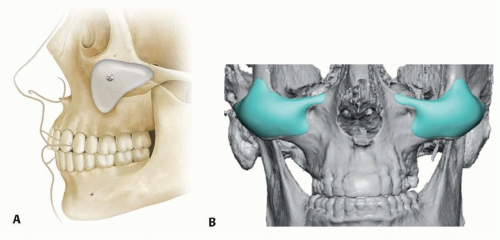 FIG 2 • A,B. Malar implant position on bony skeleton. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Physical examination should analyze both skeletal and soft tissue components, as well as overall facial balance. Asymmetries should be noted and demonstrated. It is helpful to review life-sized photos with the patient to define aesthetic concerns and goals.
History should be obtained for any active or prior history of immunosuppression, connective tissue disorders, coagulopathy, facial trauma, and implanted facial hardware before surgery. Patients should also be asked regarding recent injections of neuromodulators or fillers (temporary or permanent).
Patients with excessively thin skin, history of irradiation, or sinus disease are poor candidates for alloplastic malar augmentation.
Patients may present with a desire to enhance aesthetics of other aspects of their face (ie, nose, periorbital region). The surgeon should be able to accurately diagnose malar deficiency and assess its contribution to the overall midface harmony to the patient.
Malar skeletal augmentation is not a substitute for soft tissue augmentation or repositioning.
IMAGING
In general, radiologic assessment is not needed. Size and position of malar implants are based on the aesthetic judgment of the surgeon.
In patients with significant asymmetries, CT imaging may provide an advantage of multiplane views, three-dimensional reconstruction, life-sized models, and the manufacture of custom implants.
NONOPERATIVE MANAGEMENT
Although fat grafting and synthetic filler injections are logical nonoperative techniques that may aid in restoration of soft tissue volume loss, they have a limited role in simulating the effect of increased skeletal projection.
The aging process impacts both the soft tissue and skeletal components of the malar region. Depending on patient needs, either or both soft tissue and skeletal augmentation may be appropriate to restore youthful facial contours. It is important for the clinician to be able to differentiate the two. For example, if skeletal augmentation is performed for a patient who requires soft tissue augmentation, it will result in an overly defined appearance. On the other hand, performing fat grafting or filler injections for a patient who requires skeletal augmentation will result in a spherical shape with inadequate definition.Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Technique for Ptosis Correction
Technique for Ptosis Correction
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Indications and Techniques for Short-Scar Face-Lift
Indications and Techniques for Short-Scar Face-Lift
 Technique for Ethnic Rhinoplasty Using the Open Approach
Technique for Ethnic Rhinoplasty Using the Open Approach
 Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


