Technique for Surgical Management of the Depressor Septi Nasi Muscle
Michael R. Lee
Sammy Sinno
Rod J. Rohrich
DEFINITION
Depressor septi nasi (DSN) muscle is a paired structure occasionally responsible for deformity of the nasal tip and/or columella.1
Animation deformity of the nasal tip and/or columella may result from action of the DSN. Such deformities typically include drooping of the nasal tip and/or columella on animation.
Basal aesthetic lines (BALs) are created by the lateral borders of the columella. Excess soft tissue of the columella which includes the DSN muscle may cause distortion of the BALs.2
Medial crura footplate approximation is a described multistep process designed to improve symmetry and architecture of the medial nasal base, thereby improving the BALs.3
ANATOMY
Variations of DSN anatomy have been reported in the literature, particularly with ethnicity.4
Muscular fibers of the DSN may originate from the maxillary periosteum and/or orbicularis oris muscle. Fibers may be diminutive in some patients.
Muscle fibers of the DSN course through the columella and insert on the medial crura and nasal septum.
Columella composition includes cartilage (caudal nasal septum and medial crura) and soft tissue (muscle fibers, fibroblast, collagen fibers, elastin fibers, adipocytes, and neurovascular structures).5 Muscle fibers traversing the columella are from the DSN and orbicularis oris muscle.
The caudal septum is firmly seated on the maxillary crest and does not move with contraction of the DSN. Flanking the caudal septum is the medial crura. These more mobile medial crura may descend with contraction of the DSN.
PATIENT HISTORY AND PHYSICAL FINDINGS
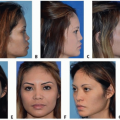
Patients may report (1) tip descent on animation, (2) short upper lip on animation, (3) transverse crease in the mid-philtral area, (4) infratip/columellar decent on animation, and (5) columellar fullness and nostril deformity on basal view.
Exam includes inspection of the nose in all classic rhinoplasty views. Inspection is initially performed in repose and then again with animation. Animation includes smiling and speaking.
Frontal view is used to evaluate tip position both in repose and with animation. The tip is inspected to determine if descent is occurring or if the misconception of tip descent is occurring. Tip position in relation to the ala and cheek during animation helps to differentiate between the two deformities. The tip is inspected both in isolation and in comparison to the nasal ala and cheek mound. It is important to determine if the tip is truly descending or if elevation of the ala/cheek mound with subnasale repositioning are responsible for the deformity. The latter is an illusion of tip descent.6 The infratip lobule is also studied to identity fullness and/or asymmetry.7 Inspection of the upper lip for shortening and/or a transverse crease is also done.
The lateral view is studied in repose and animation to study tip position, infratip architecture, and the alar-columellar relationship. Inspection of the nasal ala and check mound in relation to tip position is studied on animation. This lateral view allows a more focused inspection on the tip alone with animation. The alar-columella relationship is also assessed to identify the presence of alar retraction or a hanging columella. Fibers of the DSN attach to the mobile medial crura, and animation may distort the columella on animation.
Basal view evaluation focuses on identifying and classifying columellar deformity. Four types of deformity exist all based on the underlying anatomy.2 Excess or malpositioned cartilage and/or soft tissue can create a deformity in this area and distort the BALs.2 Comprehensive evaluation of the nasal base and in particular the medial nasal base (columella) is important when treating the DSN.
IMAGING
Imaging is typically not utilized for diagnosis of animation deformities.
3D imaging is used to discuss existing static deformities and illustrate anticipated surgical results. Many patients with the aforementioned complaints will receive increased tip rotation and placement of a columella strut to stabilize the nasal tip. These potential changes can be illustrated using an imaging system.
Changes in alar-columellar relationships are also illustrated using the imaging system.
SURGICAL MANAGEMENT
Proper diagnosis is essential for effective surgical treatment. Treatment of the DSN can be perceived as a static problem, dynamic problem, or both.2,4
Excess muscle volume can disrupt aesthetic ideals of the medial nasal base creating a static lateralization of the BALs. Surgical management focuses on reduction of the DSN and adjacent soft tissue.
Treatment of dynamic problems is deformity specific. Tip descent is managed with disruption of the DSN and stabilization. Illusion of tip descent is treated with increased rotation and stabilization. A shortened upper lip and/or transverse crease is addressed with treatment of the muscle and mucosal rearrangement.1Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Technique for Ptosis Correction
Technique for Ptosis Correction
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Indications and Techniques for Short-Scar Face-Lift
Indications and Techniques for Short-Scar Face-Lift
 Technique for Ethnic Rhinoplasty Using the Open Approach
Technique for Ethnic Rhinoplasty Using the Open Approach
 Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


