Chapter 14 Technique for Harvesting a Mid-Third Patella Tendon Graft for Anterior Cruciate Ligament Reconstruction
Skin Incision
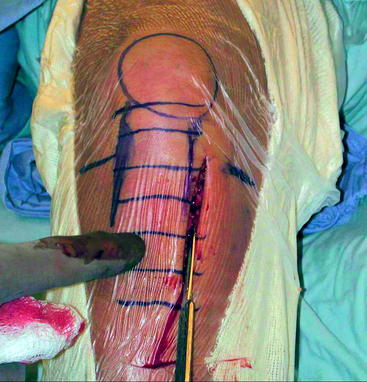
A vertical skin incision is made medial to the tibial tubercle approximately 0.5 cm medial to the medial edge of the patella tendon (Fig. 14-1). The upper end of the incision begins near the level of the joint line. The incision is extended distally to the level of the lower end of the tibial tubercle, approximately 6 to 8 cm below the joint line. Do not place this vertical incision in the midline of the knee: this leaves an unsightly scar, and it is difficult to reach the tibial tunnel from this midline position. This anteromedial incision is placed distally, which is necessary to allow positioning of the tibial guide and drilling of the tibial tunnel (Fig. 14-2). It is not necessary to extend the incision very far proximally beyond the level of the joint; when the knee is extended and a single spike retractor is placed at the superior pole of the patella, the patella is pushed distally. The patella can thus be reached through this short, distally placed incision.

Exposure
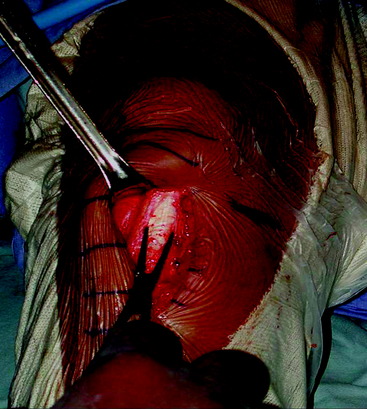
Incise the deep fascial layer lengthwise over the center of the underlying patella tendon. This deep fascial layer is thin but becomes even thinner over the tibial tubercle. Divide the deep fascial layer proximally to the level of the upper portion of the patella (Fig. 14-3). This exposes the underlying patella, patella tendon, and tibial tuberosity. Enlarge the prepatella bursa to gain access to the patella.
Taking the Graft
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


