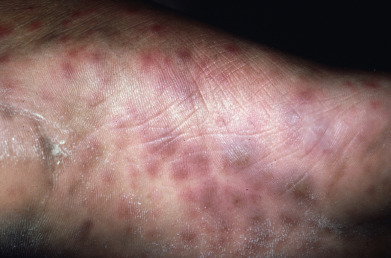
Syphilis has been dubbed “the great imitator” for its ability to assume varied morphologies. Primary syphilis is characterized by a chancre—a minimally tender, indurated ulcer—or less commonly by syphilitic balanoposthitis. Secondary syphilis can present with indurated, ham- to copper-colored papulosquamous lesions with peripheral adherent scale, annular and gyrate lesions, patchy alopecia, and gray indurated mucous patches. The palms and soles may be involved. Tertiary syphilis is characterized by destructive granulomatous disease that often involves the central face, causing destruction of the nasal bridge. Congenital syphilis can present with periostitis leading to saber shins and frontal bossing, mucositis, and gray fissured periorificial mucous patches. Vesiculobullous lesions may be seen in congenital syphilis. Pustular and crusted lesions characterize lues maligna and rupioid syphilis, respectively.
A high index of suspicion is required, and serologic testing can be falsely negative (prozone reaction) as a result of very high antibody titers. Recognition of morphologies suggestive of syphilis should prompt appropriate testing to include a skin biopsy.