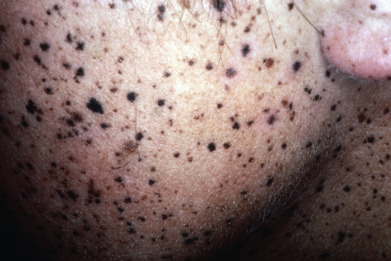
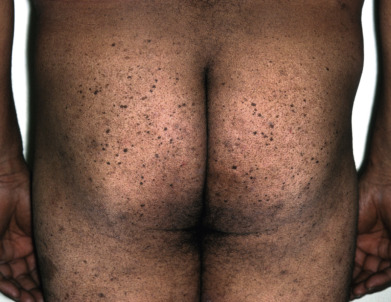
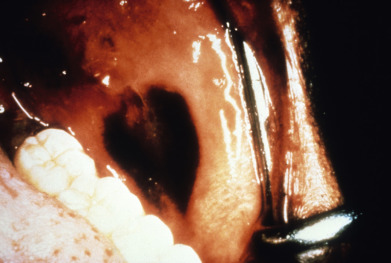
The evaluation of pigmented lesions is one of the most important skill sets in dermatology. The incidence of melanoma continues to increase, and early diagnosis plays a critical role in reducing mortality, morbidity, and the cost of health care. Melanocytic lesions may be distributed anywhere on the body, and certain lesions, such as the so-called zosteriform lentiginous nevus follow a segmental blaschkoid distribution, suggesting genetic mosaicism. Most benign lesions are round to oval, relatively small, evenly pigmented, and stable in appearance. In contrast, malignant lesions are often asymmetric with an irregular border, uneven pigmentation, larger diameter, and evolve over time. It should be noted that these concepts apply mainly to primary lesions, as metastatic lesions are often spherical and symmetric in all dimensions. The “ABCDs” of melanoma are a useful tool for education of the lay public, but only serve to identify some lesions of potential concern. They often miss amelanotic, symmetric, and evenly pigmented tumors and do not substitute for a dermatologist’s global assessment of the lesion. They should never be used as the sole criteria for biopsy or for referral to a dermatologist.
Dermoscopy allows the physician to see lesion characteristics not visible on routine examination, and confocal microscopy offers the potential for in vivo microscopic imaging of some lesions. Ultimately, though, careful visual examination of the patient’s skin remains the key initial step in identifying lesions of concern.