CHAPTER 27 Suture suspension for face and neck
History
Nature provides us with many barbed structures; such as the honeybee stinger, the woodpecker tongue and the porcupine quill; all can penetrate but defy being withdrawn. These barbs are all in one direction. In the early 1960s, Alcamo advanced the prehistoric inventions of a barbed fishing hook and arrowhead when he proposed a unidirectionally barbed suture.
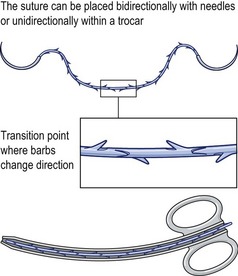
In the early 1990s Ruff developed a bidirectional barbed device (Fig. 27.1), as well as its means of manufacture and method of use. Placed by a cannula or by needles deployed in opposite directions, one set of barbs anchors the other and eliminates the need to tie a knot to secure the end. The potential advantages over a knotted loop include less ischemic necrosis, greater surgeon control of tissue approximation, more speed and obviation of the manifold problems of the knot itself. The ability to realign tissues along the array of barbs may not only be used to compress the edges of a wound together, but also to reverse the ptosis associated with aging and weight loss. In the late 1990s, Drs. Harry Buncke and Marten Sulimanidze independently described similar concepts. The USFDA approved the use of barbed sutures for tissue suspension and approximation in 2003.
Anatomy
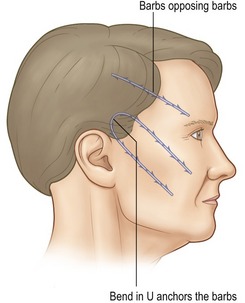
The force applied to the barbs in the face must be countered by an equally forceful opposite one. If the respective ends go in opposite directions, only half the barbs lift the face. In a U-shaped configuration, all the barbs engage the target and so this is more commonly used (Fig. 27.2).
The forehead
The suture is anchored under the galea and extends toward the brow in the deep subcutaneous fat (Fig. 27.3). It is important to avoid placing the suture deep to the frontalis in the loose areolar plane because it will elevate the brows poorly and may “click” when the frontalis contracts. The vector of the lift is reviewed as the patient looks in the mirror.
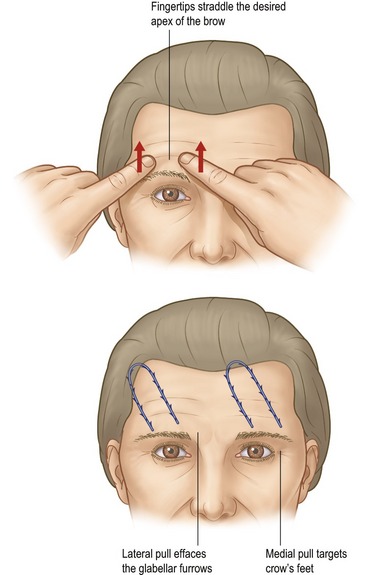
The supraorbital notch should be avoided, lest traction cause dysesthesias.
The midface
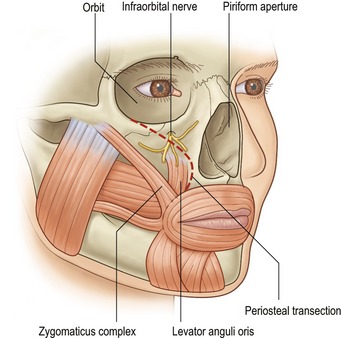
Excellent anchorage is provided by the deep temporal fascia. The barbs then extend more superficially in the SMAS and most distally in the malar fat pad. Placed more deeply, the sutures can retract the elevated malar periosteum and with it the origins of the zygomaticus and levator anguli oris muscles. If the periosteum is adequately released medially, this maneuver will elevate the oral commissure (Fig. 27.4). The barbs should not extend past the nasolabial fold where they will engage the orbicularis oris and so reduce traction on the malar fat pad. Rare instances of lower lid edema behoove the surgeon to stay inferior to the malar septum, though the reason for this occurrence is unknown. A practical guideline is to remain deep to the cheek, not eyelid skin.
The lower face
The more vertical the lift of the jowls, the tighter the neck. However, the caveats regarding excess lower lid skin which pertain to the midface also apply here. If a more horizontal vector is warranted, anchorage inferior to the deep temporal fascia is provided by the immobile SMAS and parotid capsule. As with the nasolabial fold, the barbs should not pass medial to the labiomental fold. They may extend over the mandibular border without distortion as long as the suture remains at the same depth below the skin as it courses into the neck.
Physical evaluation
• The skin laxity should be at least mild. Greater laxity warrants more mobilization, and hence dissection.
• Moderately thick subcutaneous fat provides concealment without excessive weight.
• Thin foreheads might reveal buckling when the frontalis contracts, so the vector of lift should be oblique to the muscle’s fibers.
• Median platysmal bands require transection for the best result.
• Fine wrinkles and dyschromia which warrant resurfacing should be treated at the time of the lift where feasible.
• Excess fat can be removed from an area with liposuction and immediately secured with a barbed suture. Like resurfacing, this should be done with the lift so the resulting collagen is created with the tissues the rejuvenated position.
• Tear troughs will improve with midface lifting, reducing the need to remove or reposition lower lid orbital fat.
• Lower lid skin excess can be created by elevation of the mid or lower face.









