CHAPTER 13 The multi-vectored rhytidoplasty
The stigmata of facial aging are well known. They include loss of elasticity and laxity of the cheeks, jowl formation, perioral wrinkles, platysmal bands, and laxity of cervical skin. The possible combinations are infinite, and each patient must be carefully analyzed to formulate a treatment plan. Our challenge as plastic surgeons is to recreate harmony between facial regions and to balance and smoothly blend the transition between these regions. It is important to ascertain what patients looked like early in their lives. Several questions then arise for the plastic surgeon. Do the patients themselves remember? Do we restore their youthful appearance? Do we make them look different, or even better? It is also important to keep in mind that not everyone needs to have everything corrected.
My goals in choosing a procedure for facial rejuvenation are:
• It must provide reproducible results with repeated use.
• It must allow familiarity with easily mastered techniques.
• It must be able to be performed in a reasonable time at a reasonable cost.
• It must meet the patient’s goals.
• The technique must be equally applicable for primary and secondary procedures.
 xylocaine with 1 : 200,000 epinephrine.
xylocaine with 1 : 200,000 epinephrine.The facialplasty is begun by undermining the right side of the face and neck and then the left side. The submental, anterior, and lateral aspects of the neck are undermined and defatted as necessary. Bands may be excised vertically and/or transected transversely (inferiorly), and then the SMAS in the left and right cheeks and neck is tightened. Finally, the submental incision is closed and the flaps on the right and left sides of the face and neck are redraped, the excess skin is excised and the incisions are closed. The incisions must be placed so that they will heal well, and great attention to technique and detail will result in scars that will be almost imperceptible. It does not matter how long the scar is, it matters where it is, and how it looks! (see Fig. 13.1).

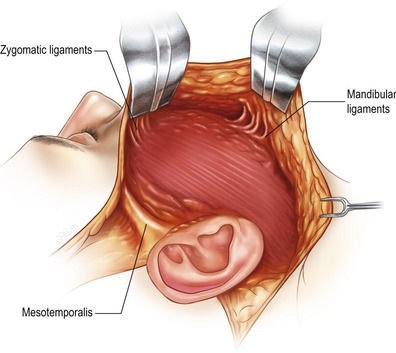
Laxity in the lower face and submental areas develops because of loss of support from the SMAS, and especially because of loss of elasticity of the skin and its attachments to the deeper tissues, except where attached to the facial skeleton by the osseocutaneous ligaments. These ligaments do not become lax with time and are the cause for some of the deformities seen in the aging face due to the descensus of the soft tissues, such as the lateral perioral labiomandibular creases and formation of jowls. Therefore it is important to release the zygomatic and mandibular osseocutaneous ligaments (see Figs 13.2, 13.3, and 13.4).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


