CHAPTER 68 Belt lipectomy: Lower body lift
Physical evaluation
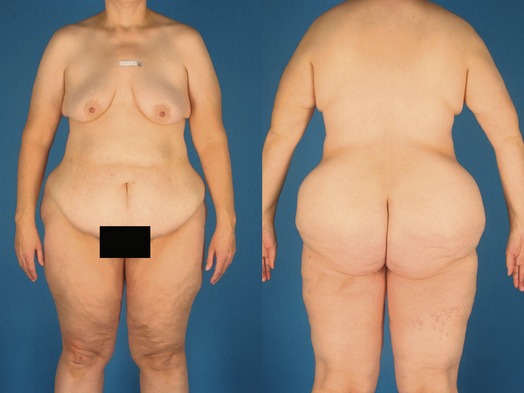
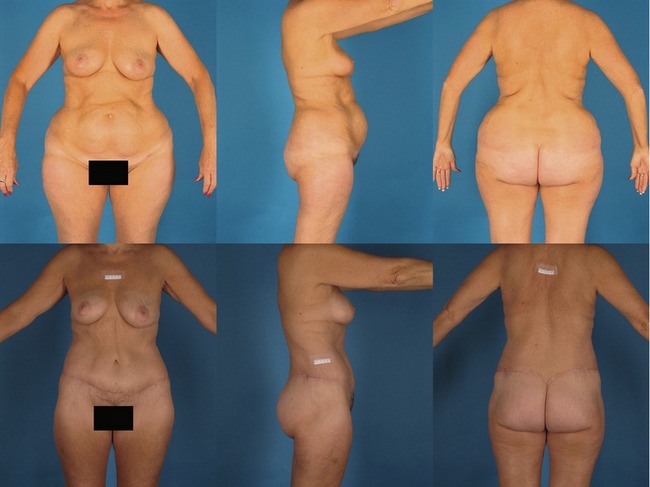
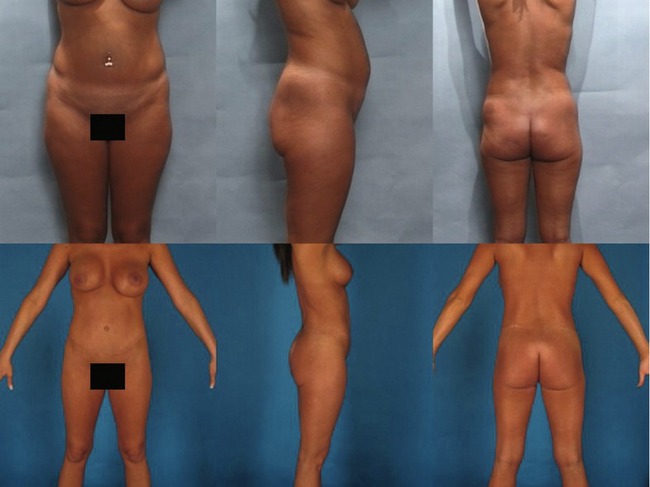
Patients who present for circumferential body lifts are most commonly massive weight loss patients. However two other groups can benefit and they include women who are 20 to 30 pounds overweight and are unable to lose that weight (Fig. 68.1), and a group of normal weight women who desire a remarkable improvement in their overall lower truncal contour (Fig. 68.2). Most of our comments here address the massive weight loss patient, who makes up 90% of patients who undergo belt lipectomy in our practice.
A complete history is taken and physical exam carried out, emphasizing:
• Weight loss history including which bariatric procedure if applicable.
• Length of time weight has been stable; at least 3 to 6 months prior to considering body contouring.
• Recording the highest and presenting body mass index (BMI) calculated by dividing the patient’s weight in kilograms by their height in meters squared.
• Rule out active medical and psychological problems and obtain a psychological clearance for surgery.
• Check that intra-abdominal content has decreased enough to allow abdominal wall plication to flatten out the abdomen.
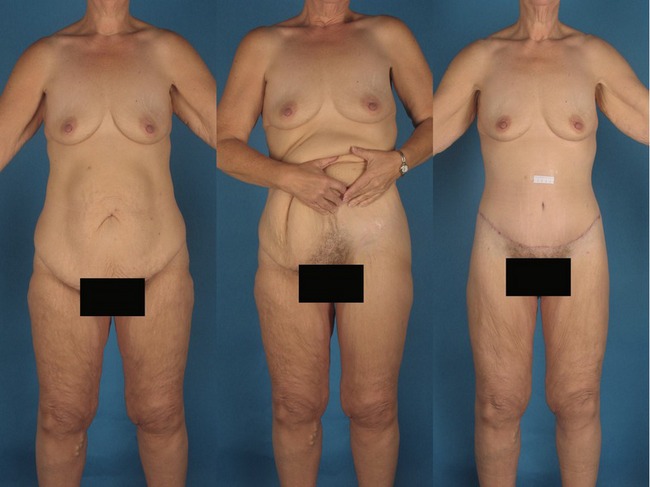
• Evaluate the extent of tissue movement by pinching the truncal tissues and determining how far away from the proposed area of resection the effect will translate, a process we call “the translation of pull” (Fig. 68.3).
• Extensive set of laboratory examinations that target post-bariatric nutritional deficiencies such as iron, total protein, albumin, calcium, etc.
• Discuss extensively the risks and complications of the surgery.
Anatomy
To understand how tissues act under the burden of massive weight loss it is important to understand the “zones of adherence”. These zones act as hooks upon which tissues hang. They vary in strength with strong adherence located at the sternum, midline of the back, the femoral/inguinal region and a zone located between the hip and lateral thigh fat deposits. A variable amount of adherence is located in the suprapubic region.
The presentation of the massive weight loss patients is quite variable and it depends on the BMI, the fat deposition pattern, and quality of the skin–fat envelope. The abdomen or back may have multiple rolls, one roll, or no rolls and a redundant ptotic mons pubis, usually with both vertical and horizontal excess. The entire lower trunk has an inverted cone appearance in almost all massive weight loss patients (Fig. 68.4). Usually the buttocks are both ill-defined and ptotic; sometimes deflated and sometimes overprojected.