8Surgical Treatment of Temporal Migraine Headaches (Site II)
Bahman Guyuron
Salient Points
• It is important to differentiate between the migraine headaches (MHs) arising from the main zygomaticotemporal branch of the trigeminal nerve (ZTBTN) and its branches, and those triggered from the anterior branch of the auriculotemporal nerve.
• The ZTBTN emerges from the deep temporal fascia approximately 16 to 17 mm lateral and 6 mm cephalad to the lateral canthus.
• The surgery could be performed under local or general anesthesia, but the latter is preferred when dealing with the main nerve and the former is better for the MHs arising from the branches of this nerve.
• This surgery is done endoscopically through two radial incisions, 1.5 cm in length and about 3–3.5 cm apart, with the medial/cephalad incision being placed about 7 cm from the frontal hairline midline and the second incision about 10-10.5 cm from the midline.
• The area is infiltrated with lidocaine containing 1:100,000 epinephrine.
• The most lateral/caudal incision is made first, deepened to the deep temporal fascia and then blindly dissected with an Obwegeser periosteal elevator sufficient enough to accommodate the Endoscopic Access Devices (EADs).
• The EADs are placed through these two incisions.
• The dissection is extended medially between any fatty tissues and the deep temporal fascia under direct visualization until the ZTBTN and the associated vessels are exposed. No fat is left on the deep temporal fascia during this dissection to assure the safety of the frontal branch of the trigeminal nerve.
• The nerve is either avulsed gently with a grasper or decompressed by enlarging the fascial opening and cauterization and removal of the concomitant vessels.
• For patients older than 30 years, the tissues are suspended laterally from the deep temporal fascia with a 3-0 PDS suture.
• The incisions are closed using 5-0 Monocryl and 5-0 or 6-0 plain catgut.
8.1 Introduction
Temporal migraine headaches (MHs) can arise from the main zygomaticotemporal branch of the trigeminal nerve (ZTBTN) and its branches, or could be the consequence of irritation of the anterior branches of the auriculotemporal nerve. These variations require totally different management. Thus, the differential diagnosis between the origins of these MHs is crucial. For the surgical treatment of auriculotemporal MH, please refer to Chapter 11.
The ZTBTN-related MHs typically arise from an area centered approximately 16 to 17 mm lateral and 6 mm cephalad to the lateral orbital commissure. Almost invariably, there is a hollowed area that can be detected by palpation at the site where this nerve exits from the deep temporal fascia. The posterolateral branch of this nerve could be irritated by the anterior branches of the superficial temporal artery (Site V), causing headaches in the temple close to the sideburn rather than the area mentioned earlier. Surgical management of these headaches is very different and will be discussed later.
8.2 Surgical Technique
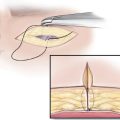
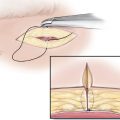
The ZTBTN is approached through two radial incisions, one placed approximately 7 cm from the frontal hairline midline and the other 3.5 cm posterolateral and caudal to the first incision (10–10.5 cm from the midline incision). Each of these incisions will be approximately 1.5 cm long and 0.5 cm behind the side-burn or temporal hairline (►Fig 8.1). While this operation can be done under local anesthesia, it is ideally performed under general anesthesia, especially if the intention is to avulse the nerve. After the incisions are designed, the temple is infiltrated with lidocaine containing 1:100,000 epinephrine. The hair is braided or gathered in a hemostat to facilitate the dissection. The incisions are made using a number 15 blade. The dissection is deepened to the deep temporal fascia using a pair of baby Metzenbaum scissors. It is crucial to identify the fascia first. For the beginner, it could prove helpful to make a small rent in the deep temporal fascia and visualize the temporal muscle to ascertain the identity of the deep temporal fascia. Using an Obwegeser periosteal elevator, the dissection is extended around the incision immediately superficial to the deep temporal fascia. The Endoscopic Access Devices (Applied Medical Technology, Cleveland, OH) are inserted to create access for the endoscopic tools and to isolate the wound from scalp hair (►Fig. 8.2). The dissection is then continued medially, visualizing the site through the scope (►Fig. 8.3). Being in the right plane is crucial to the successful identification of the ZTBTN and avoidance of injury to the frontal branch of the facial nerve. The dissection is continued medially in the plane immediately superficial to the temporal fascia directed toward the lateral orbital rim where the nerve can be found. For the beginner, it may also be helpful to tattoo, through the surface landmark passing the needle deep enough to reach the temporalis fascia, the point where this nerve commonly emerges from the deep temporal fascia (16-17 mm lateral and 6-7 mm cephalad to the lateral canthus) using methylene blue or brilliant green.1 One can then find the tattoo mark endoscopically to help locate the nerve. Even leaving the 25-gauge needle that has been passed percutaneously at the site while the dissection is being conducted endoscopically may facilitate finding the ZTBTN. It is important to realize that sometimes this nerve may have two and rarely three branches. It is for this reason that, in our view, surgery on this site through an upper eyelid incision may pose limitations. One has to explore the area sufficiently to assure that there are no additional branches.

Related posts:
 Evidence for Efficacy of Migraine Surgery
Evidence for Efficacy of Migraine Surgery
 An Overview of Migraine Headaches
An Overview of Migraine Headaches
 Detection of Migraine Headache Trigger Sites
Detection of Migraine Headache Trigger Sites
 Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
 Surgical Treatment of Frontal Migraine Headaches (Site I)
Surgical Treatment of Frontal Migraine Headaches (Site I)
 Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


