7Surgical Treatment of Frontal Migraine Headaches (Site I)
Bahman Guyuron
Salient Points
• Fifty-six percent of patients with migraine headaches (MHs) experience frontal MH.
• The headache-starting site usually corresponds to the anatomical position of the supraorbital and supratrochlear nerves.
• It is of utmost importance to assure that the MHs arising from the forehead are independent and are not an extension of the retrobulbar MH.
• The patients with frontal MHs usually have deep frown lines, may experience tender spots along the course of the related nerves, and often respond to the nerve blocks and injection of botulinum toxin A favorably.
• Computed tomography (CT) scan of the perinasal sinuses may demonstrate the presence of a main or an accessary supraorbital foramen or both.
• On patients with isolated frontal headaches, surgery is often done through a transpalpebral approach.
• On patients with a combination of frontal and temporal MHs, the endoscopic approach is preferred unless the patient has a long forehead or there is male pattern baldness, in which case the temple surgery is performed endoscopically and the frontal surgery is done through the palpebral approach.
• The transpalpebral approach is the workhorse of frontal MH surgery and is done under sedation or general anesthesia.
• The incision is placed in the most caudal supratarsal crease.
• The initial dissection is between the orbicularis and the orbital septum.
• The supraorbital nerve branch exiting the corrugator muscle is identified first.
• The muscle is removed as thoroughly as possible, saving the nerves.
• The nerves are isolated and the concomitant arteries are cauterized and transected.
• The foramen is unroofed with an osteotome or rongeur, if present.
• Fat graft or fat injection is used to replace the removed muscle volume.
• The incision is repaired using 6-0 fast-absorbing catgut.
• The endoscopic approach requires placement of five or six endoscopic access devices.
• The dissection is subperiosteal.
• The muscles are removed as thoroughly as possible with a grasper while these muscles are pushed against the grasper externally with the nondominant index finger.
• The rest of the procedure is carried out similar to the transpalpebral approach.
• Fat is harvested from the area above the zygomatic arch deep to the deep temporal fascia during the combined technique.
• On patients older than 35 years, the soft tissues are pulled laterally and the superficial temporal fascia is suspended from the deep temporal fascia with a single 3-0 PDS suture for each side.
7.1 Introduction
One of the most common migraine headache (MH) trigger sites is the forehead and 56.6% of patients have the frontal area as a component of their migraine complex. The patients may initially describe a diffuse headache over the entire frontal region. However, with examiner persistence, the patients can often identify the areas from where the headaches start more narrowly. This site commonly corresponds to the supratrochlear and supraorbital nerves. It is crucial to assure that the headache experienced in the frontal region is not an extension of a headache arising from the nose, sinus, or temple. Asking the patient if the frontal headaches can be experienced independent of the other trigger sites can elucidate whether the experienced MHs in the forehead area are triggered primarily from the forehead or are the extension of temporal or retrobulbar headaches to the supraorbital and supratrochlear nerves.
The frontal MHs often begin in the afternoon following a stressful day. These headaches commonly spread across the entire forehead. Rarely, the pain can be limited to the deep branches of the supraorbital nerve and could be confined to a small area close to or even within the hairline laterally along the course of this branch or in an isolated spot. Similarly, pinpoint headaches can be experienced by the patients along the course of the supratrochlear nerve. Almost invariably, when these sites are identified by the patient’s fingertip, a Doppler signal can be detected on the site.
The patients with diffuse frontal headaches often have strong frowning muscles with deep frown lines in repose, which get deeper with animation. Commonly, one can elicit tenderness in this trigger site. Additionally, a nerve block may produce very meaningful information, should the patient have pain at the time of examination. Many of the patients with frontal MH respond very favorably to the injection of botulinum toxin A.
Computed tomography (CT) scan findings related to this site include the presence of a main or accessory supraorbital foramen, rather than notch, where the patient usually has the most intense headaches. This is commonly the consequence of irritation of the nerve by the supraorbital vessel, triggering the MH cascade. Confinement of the nerve and vessel to a very tight space could account for the high intensity of the headache in this site even if the headaches are arising from another site, along the course of this nerve. The CT scan of the perinasal sinuses could be useful in detecting the foramen, accessary foramen, or both.
7.2 Surgical Technique
Should the patient have isolated frontal MH, which rarely occurs, the surgical procedure can be done through a transpalperbral1 or endoscopic approach.2 Even in the presence of combined temporal and frontal MH, the frontal portion of the surgery could still be carried out through an eyelid incision while the zygomaticotemporal branch of the trigeminal nerve is addressed endoscopically. This also offers an opportunity to explore the supraorbital area endoscopically using the temporal ports. Patients with a receding hairline, congenital long forehead, or those with a round and protruding forehead or proptosis would especially be suitable candidates for the transpalpebral approach.
7.2.1 Transpalpebral Deactivation of Frontal Migraine Headaches
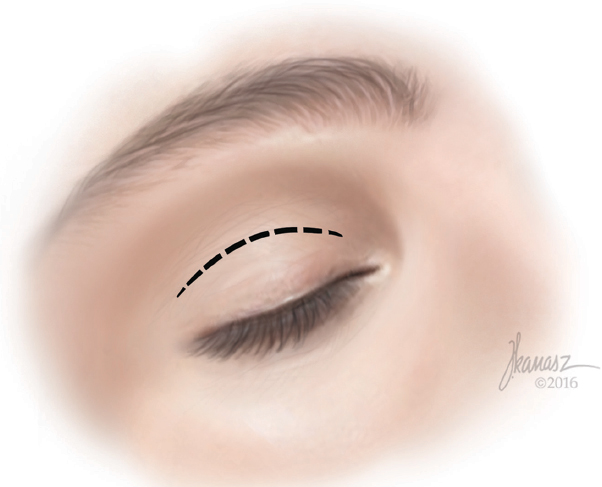
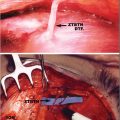
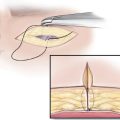
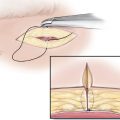
This procedure, which I developed initially for rejuvenation of the forehead on patients with optimal eyebrow position and overactive corrugator muscles, has become the workhorse of frontal migraine decompression.1 The procedure is done under general anesthesia or deep sedation. If a blepharoplasty is being done at the same time, the conventional blepharoplasty is designed. The most caudal crease is marked first. The second incision will incorporate the redundant skin, and these are joined medially and laterally, placing the lateral incision in the crow’s feet line. if no blepharoplasty is intended, the incision will be limited to the inner half of the conventional blepharoplasty incision in the most caudal supratarsal crease (►Fig. 7.1). The upper eyelid and glabellar areas are generously infiltrated with lidocaine hydrochloride containing 1:100,000 epinephrine. The eyelid skin incision is made and extended through the orbicularis muscle (►Fig. 7.2). The orbital septum is retracted caudally and the orbicularis muscle is pulled cephalically. The easily identifiable plane between these two anatomic structures is entered, and the dissection is continued toward the superior orbital rim using the cautery initially (►Fig. 7.3). The dissection is continued with a pair of baby Metzenbaum scissors, spreading the tissues parallel to the muscle fibers (►Fig. 7.4). While the orbicularis muscle is being elevated anteriorly, the depressor and corrugator supercilii muscles are exposed immediately cephalad to the orbital rim. The depressor supercilii is further dissected medially and laterally (►Fig. 7.5). This muscle is removed using the coagulation power of the cautery (►Fig. 7.6). There is a consistent large branch of the supraorbital nerve emerging from the corrugator supercilii muscle. The nerve branch is followed deeper in the muscle with a mosquito hemostat (►Fig. 7.7). The corrugator supercilii muscle is then lifted to locate the point of entrance of the nerve to the muscle (►Fig. 7.8) and the muscle is removed using the coagulation power of the electrocautery as thoroughly as possible (►Fig. 7.9). Occasionally, a gentle traction may be sufficient to avulse the muscle, but this should not be a deterring factor in radical removal of the muscle. The lateral fibers of the procerus muscle are also removed conservatively until the supratrochlear nerve is denuded. Both supratrochlear and supraorbital vessels are removed and the fascia across the supraorbital notch is released, or if there is a supraorbital foramen, it is unroofed with an osteotome or rongeur (►Fig. 7.10). At this point, a piece of fat is harvested from the medial portion of the upper eyelid, if protruding, and placed into the space created by the resection of the corrugator muscles. The fat graft is fixed to the underlying periosteum using 6-0 Vicryl or Monocryl to prevent postoperative dislodgement of the fat caudally (►Fig. 7.11). The eyelid skin is repaired using 6-0 plain catgut in a running subcuticular fashion, and the incision is treated with bacitracin ointment (see ►Video 7.1). Should there not be sufficient amount of fat in the medial compartment of the upper eyelid, 1 cc of fat is aspirated from the abdomen and injected in the muscle site as superficially as possible.
Related posts:
 Evidence for Efficacy of Migraine Surgery
Evidence for Efficacy of Migraine Surgery
 An Overview of Migraine Headaches
An Overview of Migraine Headaches
 Detection of Migraine Headache Trigger Sites
Detection of Migraine Headache Trigger Sites
 Surgical Anatomy of the Temporal Migraine Headaches
Surgical Anatomy of the Temporal Migraine Headaches
 Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
 Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


