2An Overview of Migraine Headaches
Hossein Ansari
Salient Points
• Migraine headache is the most common neurological disorder and one of the most common pain conditions, in addition to being the third most common and eight most disabling disease in the world.
• In the 2010 Global Burden of Disease Study, migraine had a global prevalence of 14.7%.
• About 11.7% of population suffer from migraine and the condition is more common in females (prevalence rate of 17.1% for females vs. 5.6% for males).
• Migraine tends to run in families and, as such, is considered a genetic disorder.
• Migraine headache incurs estimated annual costs totaling as much as $23 billion in the United States alone, including $11 billion in direct medical costs and $12 billion in lost of productivity.
• The basic physiology and underlying mechanisms contributing to the development of migraine are still poorly understood.
• While vasodilation itself may not contribute to migraine, it remains possible that vessels play a role in migraine pathophysiology in the absence of vasodilation.
• Blood vessels consist of a variety of cell types that both release and respond to numerous mediators, including growth factors, cytokines, adenosine triphosphate (ATP), and nitric oxide (NO).
• Neurons release factors such as norepinephrine and calcitonin gene-related peptide (CGRP) that act on cells native to blood vessels.
• Based on current migraine models, release of CGRP from trigeminal nerves is thought to play a central role in the painful phase of migraine due to its ability to mediate neurogenic inflammation.
• The presence of allodynia in some migraine patients, specifically chronic migraineurs, indicates that some type of “sensitization” take places during migraine.
• A peripheral mechanism with local release of inflammatory markers, which would activate trigeminal nociceptors, also probably plays an important role in this sensitization.
• Clinical presentation of the migraine can be divided into four phases including premonitory (prodromal), aura, headache, and postmonitory (resolution) phases.
• Diagnosis of migraine headaches based on ICHD-3, beta version, requires headache lasting 4 to 72 hours, and at least two of these four characteristics: unilateral, pulsating, moderate to severe, aggravated with routine physical activity, plus one of the following: nausea and/or vomiting, photophobia, and phonophobia.
• Chronic migraine (CM) is defined as headache on 15 or more days per month, for more than 3 months, in which at least 8 headache days per month fulfills the criteria for migraine described earlier.
• One important point when devising a treatment plan for the patient with chronic headache is to differentiate between chronic migraine (CM), chronic daily headache (CDH), and medication overuse headache (MOH).
• Neuroimaging, including magnetic resonance imaging (MRI) of the brain, is not a part of migraine diagnosis, and if the history is clear and the neurological examination is unremarkable, there is no need to perform any neuroimaging modality.
• Diagnosis and medical treatment of migraine headaches should be deferred to the neurologist treating the patients.
2.1 Introduction
Migraine is a brain disorder with attacks consisting of headache and other neurological symptoms. Nausea, vomiting, and/or sensitivity to light and noise often accompany “headache,” which is the most common presenting symptoms of migraines.
The clinical course of migraine is variable over the patient’s lifetime. In some patients, migraine can improve to having few or no attacks, while others might have a stable evolution and in a subset, attacks can increase in frequency over a period of time, and may become chronic.
2.2 Epidemiology and Burden
Migraine headache is the most common neurological disorder and one of the most common pain conditions, in addition to being the third most common and eighth most disabling disease in the world.1 In the United States alone, migraine accounts for approximately 5 million primary care office visits per year.2 In the more recent study from 2016, migraine and low back pain were the leading causes of Years Lived with Disability (YLDs) in high-income, high-middle-income, and middle-socio-demographic Index countries.3 In the 2010 Global Burden of Disease Study, migraine had a global prevalence of 14.7%.4
In childhood, it is slightly predominant in males, but after puberty, a 3:1 female predominance is established. Ninety percent of migraine patients have their first attack by the age of 40 years. In the United States, it is estimated that 11.7% of population suffer from migraine and the condition is more common in females (prevalence rate of 17.1% for females vs. 5.6% for males).5 Migraine tends to run in families and, as such, is considered a genetic disorder.
Migraine is a common public health and socioeconomic burden worldwide. It can negatively affect quality of life and productivity both at work and at home6 and is often underdiagnosed or misdiagnosed and undertreated or mistreated.7–9 Migraine headache incurs estimated annual costs totaling as much as $23 billion in the United States alone, including $11 billion in direct medical costs and $12 billion in lost of productivity.10,11
Despite its prevalence, the basic physiology and underlying mechanisms contributing to the development of migraine are still poorly understood and the development of new therapeutic targets is long overdue.
2.3 Pathophysiology
In 1938, Wolff and Graham suggested that the head pain of the migraine attack is produced by distension of the cranial arteries. In 1963, Wolff hypothesized the vascular theory of migraine, which for many years was accepted as the pathophysiology of migraine until the trigeminocervical (trigeminovascular) theory of migraine replaced the vascular theory. Based on this theory, activation of trigeminovascular afferents in the meninges releases inflammatory neuropeptides and other small molecules that promote neurogenic inflammation and development of peripheral sensitization of the primary nociceptive neurons. The trigeminovascular pathway conveys nociceptive information from the meninges to the brain. The pathway originates in trigeminal ganglion neurons, whose peripheral axons reaches the pia, dura, and large cerebral arteries,12 and its central axons reach the nociceptive dorsal horn laminae of the spinal nucleus V.13
The role of vasodilation in migraine is unclear and recent findings challenge its necessity. While vasodilation itself may not contribute to migraine, it remains possible that vessels play a role in migraine pathophysiology in the absence of vasodilation. Blood vessels consist of a variety of cell types that both release and respond to numerous mediators, including growth factors, cytokines, adenosine triphosphate (ATP), and nitric oxide (NO). Many of these mediators have actions on neurons that can contribute to migraine. Conversely, neurons release factors such as norepinephrine and calcitonin gene-related peptide (CGRP) that act on cells native to blood vessels. Both normal and pathological events occurring within and between vascular cells could thus mediate bidirectional communication between vessels and the nervous system, without the need for changes in the vascular tone. CGRP has been strongly linked to migraine pathology. Based on current migraine models, release of CGRP from trigeminal nerves is thought to play a central role in the painful phase of migraine due to its ability to mediate neurogenic inflammation.14
Unlike other pain states, migraine sufferers report multiple distinct triggers. These triggers are innocuous in healthy patients, which suggest that the sensitivity to different triggers in migraine is due to maladaptive changes within the nervous system. The presence of allodynia in some migraine patients, specifically chronic migraineurs, indicates that some type of “sensitization” takes place during migraine. Although it is clear that central pathology is the main reason for this phenomenon, a peripheral mechanism with local release of inflammatory markers, which would activate trigeminal nociceptors, also probably plays an important role in this sensitization.15 The key to understanding the pathophysiology of migraine is the concept of peripheral and central sensitization of trigeminal nociceptive neurons.14
In summary, the extent of these diverse symptoms suggests that migraine is more than a headache. It affects multiple cortical, subcortical, and brainstem areas that regulate autonomic, affective, cognitive, and sensory functions. Therefore, migraine is viewed as a complex, neurological disorder with a strong genetic component; headache is the most common presenting symptom of this complex condition. There is currently no objective diagnosis or treatment (cure) that is universally effective in aborting or preventing attacks.
2.4 Clinical Presentation
As discussed in the Pathophysiology section, migraine is not merely a headache, but a complex neurological disorder. Clinical presentation of the migraine can be divided into the following four phases16–18:
• Premonitory phase (prodromal): Symptoms that precede the other symptoms of the migraine attack by 2 to 48 hours and forewarn of other symptoms to come. Symptoms of this phase include a range of nonspecific complaints such as food cravings, yawning, irritability, unhappiness, euphoria, somnolence, hyperactivity, difficulty concentrating, bloating, fatigue, stiff neck, insomnia, anxiety, and so on.
Due to the nonspecific nature of these complaints, most patients do not consider them as being part of the migraine and do not report them, unless specifically asked by the physician.
• Aura phase: About 25 to 30 % of patients with migraine report transient focal neurological symptoms, which are known as aura. Migraine with aura is referred to as “classic migraine” as opposed to migraine without aura, which is known as “common migraine.” The most common type of aura is visual aura, which can present as the following:
– A shimmering arc of white or colored lights, followed by a blind spot or peripheral vision loss (scintillating scotoma).
– A zigzag appearance of lines in the visual field (fortification spectra).
– A change in the perception of the shape of viewed objects (metamorphopsia).
Other types of aura include the following:
– Sensory aura: a feeling of numbness (paresthesia), mostly unilateral, which is most common in the face (involving the tongue) and hand (chiro-oral pattern).
– Language/speech aura: presents with slurred speech, difficulty finding words or frank dysphagia.
– Motor aura: relatively rare type of aura, which presents with objective weakness of limb muscles, usually occurring unilaterally. This type of aura is mostly seen in a certain type of migraine referred to as hemiplegic migraine, which has known genetic etiology.
– Brainstem aura: presents with at least two of the following symptoms:
° Dysarthria (speech difficulty).
° Vertigo (feeling of room spinning).
° Tinnitus (ear ringing).
° Hypacusis (impairment of hearing).
° Diplopia (double vision).
° Ataxia.
° Decreased level of consciousness.
– Retinal aura: similar to visual aura, but occurs in only one eye. This type of aura is very rare.
Each individual aura symptom lasts 5 to 60 minutes and the aura is accompanied with or is followed by a headache within 60 minutes, although some individuals experience aura without headache, which is referred to and known as “migraine equivalent.” Conversely, aura does not necessarily accompany each migraine attack in patients who have migraine with aura.
• Headache phase: This is the painful phase of migraine, which catches the attention of most patients, prompting them to seek medical attention. The typical migraine headache starts unilaterally and has a throbbing (pulsating) quality. It can be associated with nausea, vomiting, and/or sensitivity to light, noise, and smell. The area of the head or neck where the headache phase starts is usually referred to as a trigger point. The location of the trigger points is extremely important when planning the treatment strategy for each individual patient.
Migraine pain can also be accompanied by abnormal skin sensitivity (allodynia) and muscle tenderness. The headache of the migraine ranges from moderate to severe and although it usually starts on one side of the head, it can later spread to involve the entire head. Also, it is not uncommon for the headache to start from more than one area at the same time. The duration of headache phase of migraine is between 4 and 72 hours. If the duration of headache attack lasts more than 72 hours (without remitting), it is classified as “status migrainosus”
As the headache progresses, it may be accompanied by a variety of autonomic symptoms (nausea, vomiting, nasal congestion, rhinorrhea, lacrimation, ptosis, yawning, frequent urination, and diarrhea), affective symptoms (depression and irritability), cognitive symptoms (attention deficit, difficulty finding words, transient amnesia, and reduced ability to navigate in familiar environments), and sensory symptoms (photophobia, phonophobia, osmophobia, muscle tenderness, and cutaneous allodynia).17
• Postdrome (resolution) phase: This is the period after the headache phase has ended and is associated with fatigue, irritability, concentration difficulty, and other nonspecific complaints.
A summary of the four phases is shown in ► Fig. 2.1.
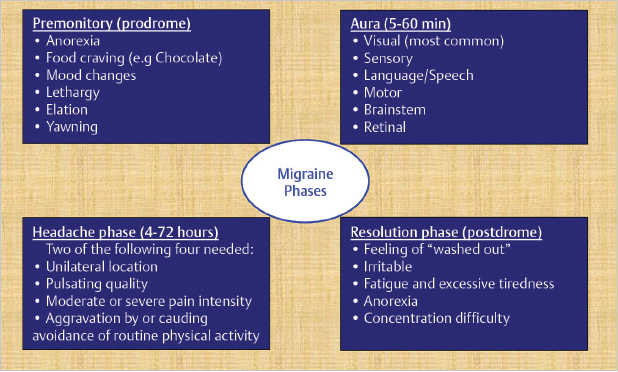
Fig. 2.1 Four clinical phases of migraine syndrome.
In order to standardized the diagnosis of headache disorders, including migraine, the International Headache Society (IHS) developed the classification, entitled the International Classification of Headache Disorders (ICHD), the first version of which was published in 1988. Since then, multiple revisions have been made in this classification and the latest edition (ICHD-3, beta version) was released in 2013.19 The ICHD provides explicit operation diagnostic rules and a common language facilitating communication on a global level.
ICHD-3, beta version, classifies migraine as follows: At least FIVE Headache attacks, each lasting 4 to 72 hours and fulfilling criteria A and B below:
A. Headache with at least TWO of the four characteristics:
1. Location: unilateral.
2. Quality: Pulsating.
3. Intensity: moderate to severe.
4. Aggravation: by routine physical activities.
B. During headache, at least one of the following two features is present:
1. Nauseas and/or vomiting.
2. Photophobia and phonophobia.
As evident, this classification and criteria are very clear and simple. This classification is available online and is easy to use by all specialties. Using these criteria can be very helpful in standardizing the diagnosis of migraine and avoiding its misdiagnosis with other headache disorders.
There are certain known triggers for migraine. Common triggers are stress, sleep disturbance, dehydration, missing a meal (fasting), alcohol (especially red wine), weather and barometric pressure changes, flickering lights, and menstrual cycles. Also certain foods such as monosodium glutamate (MSG) or nitrate containing foods, artificial sweeteners (like diet sodas) and certain smells like strong perfumes, smoke, and cleaning chemicals can trigger headache attacks in patients with migraine.
2.5 Chronic Migraine
Based on ICHD-3, beta version, CM is defined as headache on 15 or more
Related posts:
 Evidence for Efficacy of Migraine Surgery
Evidence for Efficacy of Migraine Surgery
 Detection of Migraine Headache Trigger Sites
Detection of Migraine Headache Trigger Sites
 Surgical Anatomy of the Frontal and Occipital Trigger Sites
Surgical Anatomy of the Frontal and Occipital Trigger Sites
 Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
 Surgical Treatment of Frontal Migraine Headaches (Site I)
Surgical Treatment of Frontal Migraine Headaches (Site I)
 Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


