13Surgical Treatment of Nummular Headaches (Site VII)
Bahman Guyuron
Salient Points
• Nummular headache (NH) is a disorder in which pain is localized to a specific area.
• NH is a rare disorder occurring with an estimated incidence of 6.4 to 9/100,000 in a hospital-based series.
• ICHD-3 beta describes NH as a sharply contoured pain of highly variable duration, but often chronic, in a small circumscribed area (1-6 cm) of the scalp.
• The pain is often in a round or elliptical-shaped area. It typically occurs in the parietal region and tends to be “side locked.”
• The patient can usually point to a distinct and constant spot.
• An ultrasound vascular Doppler signal can almost invariably be detected.
• A positive response to a nerve block could be extremely informative so long as the patients report headaches at the time of office visit.
• Surgery is performed under local anesthesia and involves a 5- to 10-mm incision and removal of a small vessel with or without removal of a terminal nerve branch.
• The incision is repaired with 6-0 Monocryl and 5-0 or 6-0 plain catgut depending on the site.
• Surgery almost uniformly results in elimination of headaches in the operated site.
• There is a small chance of NH developing in the vicinity of the previous surgery site, but never exactly in the same area.
13.1 Introduction
Nummular headache (NH) is a rare disorder occurring with an estimated incidence of 6.4 to 9/100,000 in a hospital-based series,1,2 nevertheless, this entity seems more common post-migraine surgery than statistics suggest. The International Classification of Headache Disorders, third edition, beta version (ICHD-3 beta) describes NH as a sharply contoured pain of highly variable duration, but often chronic, in a small circumscribed area of the scalp. The pain is often in a round or an elliptical-shaped area. While it typically occurs in the parietal region, it can be anywhere on the scalp. Over-the-counter analgesics are commonly adequate to treat most NH patients. Sometimes the pain is severe, necessitating additional modalities.3,4
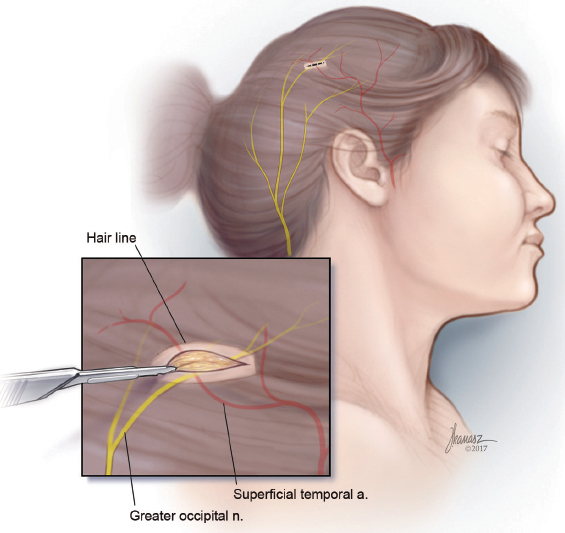
13.2 Detection of the Trigger Site
The patient is asked to point to the trigger site, and the area is marked. Almost invariably, a vascular signal can be detected with ultrasound Doppler. Occasionally, it is necessary to move the Doppler probe around a few millimeters outside of where the patient points to find the signal. The signal site is then marked. Should the patient report headache at the time of the office visit, the Doppler signal site is injected with 0.5 mL of Naropin. A positive response to a nerve block could be extremely informative as long as the patient reports having a headache at the time of the office visit. A negative nerve block does not mean that surgery will not be effective in the injected site.
13.3 Surgical Procedure
The procedure is done under local anesthesia as an office procedure in the majority of the patients. After the surgical site is identified, the marked area of pain and associated Doppler signal are injected using lidocaine 1% with epinephrine (1:100,000). A 5- to 10-mm incision is designed in the previously marked area. Usually, a 0.5-inch 30-gauge needle is used to inject slowly and with single skin penetration. After awaiting an appropriate time to maximize the anesthetic and vasoconstrictive effect of the injection, a number 15 blade is used to make an incision through the skin and dermis (►Fig. 13.1). A mosquito hemostat is used for the dissection (►Fig. 13.2). The direction of the dissection is based on the logical anatomic course of the artery and the nerve in that area. Once the artery is identified, it is dissected both proximally and distally to obtain a segment for removal (►Fig. 13.3). Larger arteries will require suture ligation using a 5-0 or 6-0 Monocryl, while smaller arteries are adequately treated using targeted cauterization. The entire intervening segment of the artery is removed. Small nerves that are intimately associated with the artery are removed (►Fig. 13.4) when detected. Larger nerves require division with the cut end buried in the muscle to minimize the potential for a neuroma formation, if a muscle is present in the vicinity of the nerve. After hemostasis is verified, and following assurance that there are no additional branches of the nerve or the artery, the incision is closed. The first stitch includes a bite of the deeper tissues to obliterate the dead space. In the hair-bearing areas, a 5-0 plain catgut suture is used, while in exposed areas, a 6-0 fast-absorbing catgut should be employed (►Fig. 13.5) (see ►Video 13.1). The incision in sites without hair is covered with waterproof dressing, which is removed in 7 to 8 days. Bacitracin ointment is used where the presence of hair can make adherence of the occlusive dressing difficult.
Related posts:
 Evidence for Efficacy of Migraine Surgery
Evidence for Efficacy of Migraine Surgery
 An Overview of Migraine Headaches
An Overview of Migraine Headaches
 Detection of Migraine Headache Trigger Sites
Detection of Migraine Headache Trigger Sites
 Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
Surgical Treatment of Auriculotemporal Migraine Headaches (Site V)
 Surgical Treatment of Frontal Migraine Headaches (Site I)
Surgical Treatment of Frontal Migraine Headaches (Site I)
 Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Surgical Treatment of Lesser Occipital Migraine Headaches (Site VI)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


