Lymphedema is a pathologic condition that results from a disturbance of the lymphatic system, with localized fluid retention and tissue swelling. Primary lymphedema is a congenital disorder, caused by a malformation of lymph vessels or nodes. Major progress has been achieved in the radiologic diagnosis of patients affected by lymphedema. The ideal treatment of the affected limb should restore function and cosmetic appearance. Surgical treatment is an alternative method of controlling chronic lymphedema. Free lymph nodes autologous transplantation is a new approach for lymphatic reconstruction in hypoplastic forms of primary lymphedema. The transferred nodes pump extracellular liquid out of the affected limb and contain germinative cells that improve immune function.
- •
The ideal treatment for lymphedema of the limbs must restore function and normal cosmetic appearance.
- •
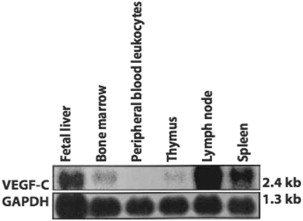
Human lymph nodes express high levels of the lymphatic vessel growth factor VEGF-c, which is responsible for stimulating lymphangiogenesis in the treated limb.
- •
Primary lymphedema can be associated with other organ malformations and genetic disorders: cancer and diseases of the central nervous system, lungs, heart, kidneys, and other organs can accompany lymphedema of sudden onset. The most prevalent hereditary disorders associated with lymphedema are Milroy disease, Meige syndrome, lymphedema-distichiasis, and yellow nail syndrome.
- •
Patients with hypoplastic forms of lymphedema on MRL are the preferred candidates for autologous lymph nodes transplantation.
- •
When the lymphedema is not too advanced, complete or near complete recovery is possible.
Introduction
The ideal treatment for lymphedema of the limbs must restore function and normal cosmetic appearance. Physiotherapy (manual drainages, pressotherapy, compression, bandages) is the usual treatment for chronic lymphedema and is considered by many as the only treatment for long-term management. It is not a curative therapy, but helps to control the evolution of the disease. Chronic lymphedema is a progressive condition, characterized by a degenerative and inflammatory process resulting in diffuse, irreversible tissue fibrosis. Surgical treatment is an alternative method of controlling chronic lymphedema.
Precise diagnosis of lymphedema has achieved major progress: lymphangiography with oil and lymphoscintigraphy were once very useful, but these examinations have important drawbacks (eg, infection, pulmonary embolism). Magnetic resonance lymphangiography (MRL) with T2-weighted imaging has greater sensitivity, and allows complete visualization of the lymphatic system without any injection.
Free autologous lymph node transplantation in hypoplastic forms of lymphedema is a new approach for lymphatic reconstruction, a more anatomic strategy compared with the multiple lymphovenous anastomoses. Recent findings on the growth hormones produced by the lymph nodes permit further understanding of the efficacy of these procedures. Three lymph node flaps can be used, depending on the affected segment and available donor sites. These flaps are located on the inguinal, thoracic, or cervical area. The transplanted nodes pump the extracellular liquid responsible for lymphedema formation, and contain germinative cells that improve immune functions ( Figs. 1 and 2 ).


Human lymph nodes express high levels of the lymphatic vessel growth factor vascular endothelial growth factor (VEGF)-c. This growth hormone is responsible for stimulating lymphangiogenesis in the treated limb. Saaristo and colleagues compared the production of this growth factor by different tissues of the immune and hematopoietic systems. Lymph nodes expressed the highest levels of VEGF-c among the tissues tested ( Fig. 3 ).
Each living node contains a plexus between the lymphatic and venous systems. The transplanted lymph nodes also probably work as a biologic lymphovenous anastomosis ( Fig. 4 ).
Clinical presentation
Alterations of lymph drainage induce stasis of the lymph and progressive tissue changes with enlargement of the subcutaneous tissue and thickening of the skin. Secondary infections, immune disorders, and cosmetic and psychosocial impairment can severely affect patients with lymphedema.
Diagnosis of lymphedema is done mainly by clinical assessment. A detailed history, clinical evaluation, and physical examination are necessary. Age of inset, episodes of infections and inflammatory attacks, previous medical treatments, and visits to tropical countries with endemic filariasis should be recorded. Transitory edema of the affected limb and a family history of limb edema should be questioned. Lymphedema is usually painless, but a sensation of heaviness of the affected limb is a common complain. Acute inset or worsening of the lymphedema can produce pain, caused by distention of the aponevrosis around the deep lymphatic system.
In the lower limbs, lymphedema is usually unilateral and, if it is bilateral, it is generally asymmetric. In young adults the lymphedema in the lower limb is unilateral in 70% of cases, and bilateral in the other 30%. The lower body, upper extremities (unilateral or bilateral), the abdomen, genital area, and trunk can be involved. The skin folds at the base of the toes and fingers are broadened. This is caused by excessive skin thickness and fluid accumulation with tissue overgrowth (Stemmer sign).
Skin changes include pinky-red discoloration, hyperkeratosis, papillomatosis, and lymph vesicles. Interdigital mycosis must be treated to prevent secondary infections. Associated venous insufficiency may cause ulcerations of the skin.
Elephantiasis can be observed in hypoplastic and hyperplasic forms, but the disorders of the skin and the multiple folds are very difficult to treat. Evolution into lymphangiosarcoma is rare, but can occur if elephantiasis is not treated.
Perimetry of the limb is an indirect assessment of its volume. It is a traditional tool to evaluate limb changes. Measurements are made at the level of the two distal major joints (knee and ankle in the lower limb), 10 and 20 cm proximal to them.
Clinical presentation
Alterations of lymph drainage induce stasis of the lymph and progressive tissue changes with enlargement of the subcutaneous tissue and thickening of the skin. Secondary infections, immune disorders, and cosmetic and psychosocial impairment can severely affect patients with lymphedema.
Diagnosis of lymphedema is done mainly by clinical assessment. A detailed history, clinical evaluation, and physical examination are necessary. Age of inset, episodes of infections and inflammatory attacks, previous medical treatments, and visits to tropical countries with endemic filariasis should be recorded. Transitory edema of the affected limb and a family history of limb edema should be questioned. Lymphedema is usually painless, but a sensation of heaviness of the affected limb is a common complain. Acute inset or worsening of the lymphedema can produce pain, caused by distention of the aponevrosis around the deep lymphatic system.
In the lower limbs, lymphedema is usually unilateral and, if it is bilateral, it is generally asymmetric. In young adults the lymphedema in the lower limb is unilateral in 70% of cases, and bilateral in the other 30%. The lower body, upper extremities (unilateral or bilateral), the abdomen, genital area, and trunk can be involved. The skin folds at the base of the toes and fingers are broadened. This is caused by excessive skin thickness and fluid accumulation with tissue overgrowth (Stemmer sign).
Skin changes include pinky-red discoloration, hyperkeratosis, papillomatosis, and lymph vesicles. Interdigital mycosis must be treated to prevent secondary infections. Associated venous insufficiency may cause ulcerations of the skin.
Elephantiasis can be observed in hypoplastic and hyperplasic forms, but the disorders of the skin and the multiple folds are very difficult to treat. Evolution into lymphangiosarcoma is rare, but can occur if elephantiasis is not treated.
Perimetry of the limb is an indirect assessment of its volume. It is a traditional tool to evaluate limb changes. Measurements are made at the level of the two distal major joints (knee and ankle in the lower limb), 10 and 20 cm proximal to them.
Related posts:
 Are We Witnessing the Emergence of a Superspecialty?
Are We Witnessing the Emergence of a Superspecialty?
 Applications of Biomaterials in Plastic Surgery
Applications of Biomaterials in Plastic Surgery
 Impact of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Impact of Reconstructive Transplantation on the Future of Plastic and Reconstructive Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


