This article summarizes the current knowledge on the new developing field of reconstructive transplantation. A brief outline of vascularized composite allografts (VCA) such as human hand, face, larynx, and abdominal wall transplants is provided. The clinical applications and indications for these new reconstructive transplantation procedures are outlined. The advantages, disadvantages, and complications and concerns surrounding clinical VCA are discussed. Finally, the impact of reconstructive transplantation on the future of plastic and reconstructive surgery is presented.
- •
Complex posttraumatic deficits can be repaired with well-established microsurgical techniques; the tradeoff includes significant donor site morbidity, lack of perfect function restoration, and less-than-optimal esthetic outcomes.
- •
Reconstructive transplantation includes vascularized composite allotransplants (VCAs), from a human donor, and involves transplantation of tissues derived from ectoderm and mesoderm.
- •
The major concern in VCA reconstructive transplantation is the need for lifelong immunosuppression to prevent graft rejection.
- •
The question remains whether reconstructive transplantation should be considered either only after all conventional options have been exhausted or as the first option after traumatic injury causing severe functional and/or esthetic deficits of the human body.
Introduction of reconstructive transplantation into plastic surgery
The past 2 decades has seen an ongoing search for new reconstructive options to restore functional and esthetic deficits of patients with severe deformities of the face, extremities, hands, and other parts of the body for which application of currently available reconstructive options resulted in less-than-optimal outcomes.
The major problem with reconstruction of complex posttraumatic deficits on the face and extremities was a lack of available tissues that resembled the injured or missing parts, such as the nose, lips, or eyelids in the case of facial deformities, or the lack of spare parts, such as joints, fingers, or hands in cases of extremity injuries involving amputations.
Conventional techniques allowed for staged reconstruction of these deformities, providing coverage, tissue expansion, and functional restoration with borrowed tissues, including free tissue transfers or a combination of all available techniques.
The well-established microsurgical techniques contributed significantly to the field of reconstructive surgery by introducing procedures such as toe-to-hand transfers, for example, in which missing functions were restored often in one surgical attempt.
The tradeoff, however, included significant donor site morbidity, lack of perfect function restoration, and less-than-optimal esthetic outcomes. In many situations, multiple reconstructive attempts were undertaken, thus limiting sources of available autologous tissues over time, and often leaving patients with the visible stigma of posttraumatic disfigurement.
Autologous free tissue transfers and replantation procedures introduced the idea of tissue transplantation as a method of functional and esthetic restoration. The major advantage of this approach was the fact that autologous transplants did not require immunosuppression to keep the grafts alive. The major disadvantage, however, was the awkward esthetic outcome of single or multiple flaps of varying color and bulkiness used for facial coverage, or the combination of flaps and short toes sticking out from deformed hands.
As a result of the lack of “specialized spare parts” that could be borrowed from the bodies to restore missing functions, the idea of reconstructive transplantation was borne and introduced to plastic surgery. It was based on more than 20 years of experimental and preclinical work testing the technical, functional, and, most importantly, immunologic aspects of reconstructive transplantation.
Plastic and reconstructive surgery embraced the new field of reconstructive transplantation using vascularized composite allotransplants (VCAs), such as human hand, face, larynx, trachea, abdominal wall, and lower extremity transplants, and included these into the armamentarium of plastic surgery.
This article discusses the current and future impact of reconstructive transplantation on the field of plastic and reconstructive surgery.
Reconstructive transplantation as an alternative surgical option
Reconstructive transplantation includes VCAs and involves transplantation of tissues derived from ectoderm and mesoderm. VCAs typically contain skin, fat, muscle, nerves, lymph nodes, bone, cartilage, ligaments, and bone marrow as opposed to a single tissue organ, which is the case in conventional solid organ transplantation. An example of VCA is limb transplantation, in which the transplanted graft includes skin, muscle, nerve, blood vessels, and bone. The function and immunologic properties of the composite tissue transplant are more difficult to define, because each individual component has its own unique characteristics that ultimately affect the successful outcome of the transplantation. Most applications of VCA predominantly improve quality of life for patients with non–life-threatening conditions and aim to restore anatomic, cosmetic, and functional integrity. The benefits gathered from these procedures must be balanced against the morbidity of the surgical procedure itself, the side effects of lifelong immunosuppression therapy, and the cost of surgery and immunosuppressive medications ( Box 1 ).
Advantages
- •
Reconstruction of VCA in a single surgical procedure
- •
No donor-site morbidity
- •
Access to the esthetic and functional units and body parts
- •
Better skin texture, pliability, and color match
- •
Restoration of form and function with “alike” body parts and components
- •
Reduced number of surgical procedures and need for general anesthesia
- •
Reduced number of postsurgery hospitalization days
Disadvantages
- •
Need for life-long immunosuppressive therapy
- •
Need for adequate matching between the donor and recipient (age, sex, race)
- •
Increased risks of comorbidities (viral and bacterial infections, lymphoproliferative disorders, diabetes, avascular necrosis of bones)
- •
Risk of acute or chronic rejection
- •
Need for the rescue protocol in the case of VCA rejection
- •
Social, ethical, and psychological issues
- •
Significant cost of immunosuppressive therapy
Advances in VCA transplantation have opened a new era in the field of reconstructive surgery. Since 1998, after the report on the first successful hand transplantation in France, the field of VCA has further developed, opening new alternatives for patients who have lost their extremities and hands.
On November 15, 2004, Dr Maria Siemionow at Cleveland Clinic received the world’s first Institutional Review Board (IRB) approval to perform face transplantation in humans. This event opened a new era in reconstructive surgery of the human face.
On November 27, 2005, in Amiens, France, a surgical team led by Drs Bernard Devauchelle and Jean-Michel Dubernard announced that they had performed a partial face transplant on a 38-year-old woman whose face had been disfigured by a dog bite. To date, a total of 19 face transplantations have been performed worldwide in France, China, the United States, and Spain.
The world’s first near-total face transplantation was performed in Cleveland in December 2008 by a team led by this author. This procedure was, until now, the most complex face transplant, involving restoration of 3-dimensional craniofacial skeleton with multiple functional units.
The patient was a 45-year-old woman who experienced severe facial trauma to her midface from a close-range shotgun blast in September 2004. Her facial deformities included absence of nose, nasal lining, and underlying bone; contracted remnants of the upper lip; loss of orbicularis oris and orbicularis oculi muscle functions; distorted and scarred lower eyelids with ectropion; right-eye enucleation supported by eye prosthesis; and facial nerve deficit manifested by the lack of midface function ( Fig. 1 ).

Before face transplantation, the patient had undergone 23 major autologous reconstructive operations that included correction of bone defects with free fibula and split-calvaria/rib grafts; soft-tissue defects with anterolateral free flap, temporalis muscle flap, paramedian forehead flap, and radial forearm free flap; and skin defects with multiple split-thickness skin grafts.
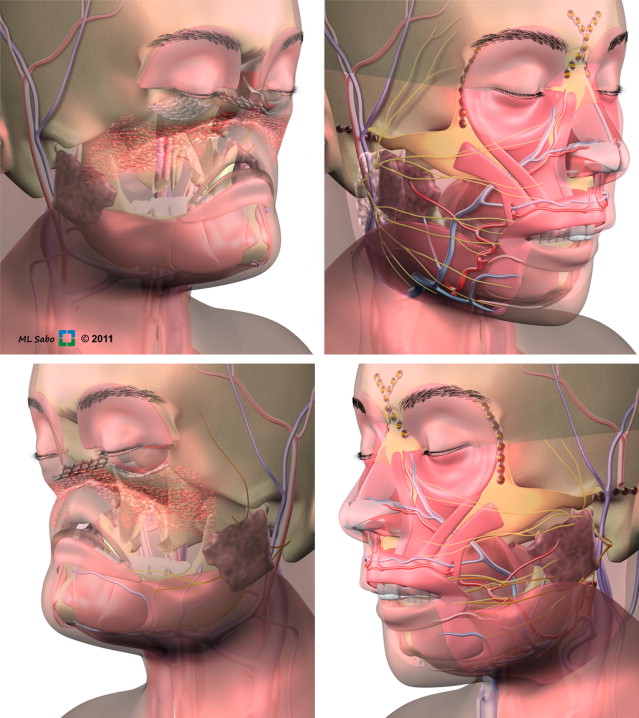
The donor was a brain-dead woman who matched the patient in age, race, and skin complexion. The allograft was designed to cover the recipient’s anterior craniofacial skeleton, and it included approximately 80% of the surface area of the anterior face. It was based on a Le Fort III composite tissue allograft containing total nose, lower eyelids, upper lip, total infraorbital floor, bilateral zygomas, and anterior maxilla with incisors, and included total alveolus, anterior hard palate, and bilateral parotid glands ( Fig. 2 ).
The allotransplant inset to the recipient started with the adjustments of a Le Fort III composite allograft to the recipient’s skeletal defect. Once bone components of the facial allograft were secured and stable, bilateral microvascular anastomoses of both arteries and veins were performed. Once the craniofacial skeleton was intact, the bilateral facial nerves were connected using standard epineural repair.
First, the donor’s vagus nerve, taken as an interpositional graft, was attached to the upper division of the trunk of the right side of the recipient’s facial nerve. On the left side, the donor’s hypoglossal nerve, used as an interpositional graft, was attached to the upper division of the trunk on the recipient’s facial nerve. Both grafts were connected to the main trunk of the donor nerve. Porous polyethylene implants were then used to reconstruct orbital floors. Finally, the lower eyelids, including the recipient’s conjunctiva and lash lines, were reconstructed bilaterally using donor eyelid skin. The composite facial allograft inset was completed after skin closure.
Face transplantation requires lifelong immunosuppression to prevent the graft from acute rejection and to support long-term survival. The protocol included induction of immunosuppression with rabbit antithymocyte globulin (1 × 2 mg/kg intravenously once a day for 9 days) in combination with methylprednisolone given as a 1000-mg bolus intravenously on the day of transplant, and rapidly tapered thereafter. The immunosuppressive regimen was maintained with tacrolimus, mycophenolate mofetil, and low-dose oral prednisone.
Functional outcomes improved over time and, after 9 months, sensory discrimination returned to the entire facial skin, as measured with the Pressure-Specified Sensory Device (N K Biotechnical Engineering, Golden Valley, MN), indicating the presence of 2-point sensory discrimination at the area under the lower eyelids, upper lip, and the tip of the nose on both sides of the graft. Motor recovery included improved facial mimetics with asymmetric smile and upper lip occlusion.
The functional recovery of this 3-dimensional facial defect is excellent, with restoration of major functions, such as eating solid food without the need of a gastric tube, drinking from a cup, and reestablishment of intelligible speech after hard palate reconstruction with composite allograft and palatal obturator support.
At 3 years after transplant, the aesthetic outcome has been improved through excision of the redundant skin and subcutaneous tissues ( Fig. 3 ). Psychologically, the patient is doing well, without symptoms of depression or posttraumatic stress disorder. Finally, her pain level has been significantly reduced, because the scarred and contracted tissue within her face was removed during face transplantation.
To illustrate the approach undertaken by a single surgical procedure of human face reconstructive transplantation, a detailed outline of the sequence of events accompanying a reconstructive transplantation case is presented.
The presented summary of conventional approaches to reconstruct severe esthetic and functional defects illustrates the limitations of current conventional techniques and of the body to supply an adequate number and quality of tissues for such complex reconstructions. It is also clear that, despite the surgical efforts undertaken by qualified experts in the field, the outcome was less than optimal and the patient’s quality of life did not improve after more than 23 conventional reconstructions.
To overcome these difficulties and introduce innovative approaches to plastic and reconstructive surgery, reconstructive transplantation aims to restore both the esthetic and functional components of the disfigured human face in one surgical procedure. This same approach is taken for other VCA transplants, including extremities, hand, larynx, trachea, and abdominal wall allotransplantation.
The major difference between conventional reconstruction of complex body deficits and reconstructive transplantation is the privilege of access to human donors, which allows selection of perfect esthetic and functional components (eg, face, hand). Reconstructive transplantation allows compliance with Giles’ mantra of replacing “the like with the like” tissues to restore, perfectly, missing parts of the body.
In this aspect, the impact of reconstructive transplantation on the field of plastic and reconstructive surgery is unprecedented and the future development of the field of VCA is guaranteed.
Related posts:
 Are We Witnessing the Emergence of a Superspecialty?
Are We Witnessing the Emergence of a Superspecialty?
 Applications of Biomaterials in Plastic Surgery
Applications of Biomaterials in Plastic Surgery
 Robot-Assisted Plastic Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Robot-Assisted Plastic Surgery
Surgical Advances in Burn and Reconstructive Plastic Surgery
Microsurgical Advances in Extremity Salvage
The Latissimus Dorsi Detrusor Myoplasty for Functional Treatment of Bladder Acontractility
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


