Surgical Scars
John P. Tsatalis
Marina Perper
Adam S. Aldahan
Stephanie Mlacker
Keyvan Nouri
BACKGROUND
Scarring is a physiological process that acts to heal the skin following injury. In scarring, fibrous tissue fills the defect and restores the integrity of the skin. Injury, surgery, burns, acne, and infection can all create the conditions that result in scarring. Scarring can have many physical, psychological, and social effects.1 Physically, scar symptoms include pain, itching, stiffness, tenderness, and (typically in burn patients) contractures. The cosmetic appearance of scars also likely contributes to psychosocial effects that interfere with our social interactions and decrease the quality of our life. The stigma of scars is enhanced if the scar is large or in a conspicuous area.2,3
PRESENTATION
Scar formation following a surgical procedure commences from the date of surgery. Treatment of scars therefore requires prophylaxis, proper wound care, and treatment upon suture removal.
DIAGNOSIS
Clinical Diagnosis
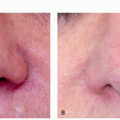
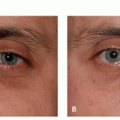
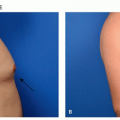
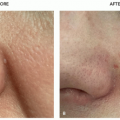
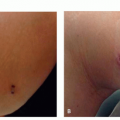
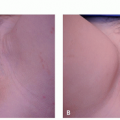
Clinically scars appear as atrophic skin-colored depressed plaques to well-circumscribed pink-red or violaceous-brown nodules with smooth surface. Hypertrophic scars remain within the borders of the original scar, whereas keloids extend beyond the margins of the original scar. Hypertrophic scars and keloids can range from soft to firm and asymptomatic to pruritic or tender. Keloids are typically found on the head, ear, neck, chest, shoulders, and arms. Often there is a history of a preceding surgical procedure, traumatic wound, burn, or acneiform papule, but keloids rarely can appear spontaneously.
Histopathology
Biopsy of nonhypertrophic scars shows fibroblasts oriented parallel to the epidermis, with perpendicular dermal blood vessels and decreased elastic fibers. Hypertrophic scars exhibit nodular morphology with
overlying epidermal atrophy and a whorled dermal proliferation of fibroblasts. Keloid scars exhibit a nodular morphology with relatively hypocellular dermal proliferation of fibroblasts and thick, densely packed, hyalinized collagen fibers. Atrophic scar histology is described in chapter 8.4.i (Atrophic Acne Scars).4
overlying epidermal atrophy and a whorled dermal proliferation of fibroblasts. Keloid scars exhibit a nodular morphology with relatively hypocellular dermal proliferation of fibroblasts and thick, densely packed, hyalinized collagen fibers. Atrophic scar histology is described in chapter 8.4.i (Atrophic Acne Scars).4
Subtypes
There are many different types of scars that occur for a vast variety of reasons. Acne scars are morphologically diverse and are commonly seen on the face, and contracture scars from burns are distinctive.5 From a surgical perspective, there are 2 main types of scars: hypertrophic and keloid. A third type, atrophic scarring, is less common and is more often associated with acne scarring.
Scar treatment algorithms vary depending on the scar type, location, and whether it has a cosmetic effect. Scars, no matter the type, are difficult to treat, and despite a broad spectrum of treatments, the recurrence rates are universally high. Still, it is possible for scars to spontaneously improve with time.3
Hypertrophic Scar
Hypertrophic scars are characterized by a widened, thickened, irregular, and elevated scar that does not extend beyond the original wound boundaries.6 After a cut or surgery, the scar is usually linear. Once the scar reaches a specific size, it ceases to grow and may even regress over time. The scar can, however, thicken for up to 6 months. Hypertrophic scars are often erythematous and cause pruritus, pain, and restriction of movement for up to several years.6 There are no familial or racial associations with hypertrophic scar formation. Most hypertrophic scars are formed in people between puberty and the age of 30 years.
Keloid
A keloid is a scar that grows beyond the boundaries of the original injury site. They are elevated, hard, smooth, amorphous scars that spontaneously form. Sometimes they arise after injury; at other times they develop months after injury and even have been found to develop without trauma. Most people never form keloids, whereas others develop them easily. Keloids are associated with pruritus and pain, even more so and at higher levels than hypertrophic scars. Keloid scar recurrence is around 50% after treatment6 (see also chapter 8.2).
Etiology
The exact cause of keloids is currently unknown; however, the trauma from surgery could catalyze the formation of a keloid scar.7 Keloids most commonly occur on the shoulders and upper back. It is thought that the tightness of skin and the increased muscle in those areas contribute to the increased frequency of keloids in these areas.6 Like hypertrophic scars, keloids are associated with adverse wound healing factors such as infection, excess tension, and repeat trauma. Keloid formation is most common in patients with more highly pigmented skin, such as blacks, Hispanics, and Asians.7 The scars are believed to be familial-linked.
Differential Diagnosis
Keloidal morphea/nodular scleroderma
Lobomycosis
Xanthoma disseminatum
Adult-onset juvenile xanthogranuloma
Dermatofibroma
Dermatofibrosarcoma protuberans
Keloidal plaques of Ehlers-Danlos IV
Trichilemmal carcinoma
Mixed tumor (chondroid syringoma)
Apocrine cystadenoma
Erythema elevatum diutinum
Infantile digital fibromatosis
PATHOGENESIS
Nonhypertrophic
The process of wound healing and eventually scar formation includes 3 overlapping phases that restore the skin. In order, the stages are inflammatory, proliferative, and remodeling.8,9 The first phase, inflammatory, takes 1 to 3 days and is characterized by hemostasis. Hemostasis is the process by which the body stops bleeding by the formation of clot composed of platelets and clotting factors. At the same time, neutrophils, macrophages, and other immune cells arrive to fight foreign particles at the wound site. The next phase is the proliferative phase and lasts from 4 to day 21. In this stage of wound healing, certain cells perform specific tasks. To restore the integrity of the skin, the cells work together; keratinocytes multiply and cover the epidermis, the outermost skin layer, in a process called re-epithelialization; endothelial cells generate blood vessels; and fibroblast cells form new collagen. The final stage of the wound healing
process, the remodeling phase, lasts from day 21 to year 1. Throughout this phase, new collagen replaces the old tissue and the wound begins to contract, prompted by myofibroblast cells. This action establishes scar formation and enhances wound strength and takes more than a year.8 Ideally, by the end of the wound healing process, the scar will form with a faint, fine skin-colored scar line without any other symptoms. Especially during the last remodeling phase, if anything goes wrong during the wound healing process, the wound may heal abnormally with pathological scarring.9
process, the remodeling phase, lasts from day 21 to year 1. Throughout this phase, new collagen replaces the old tissue and the wound begins to contract, prompted by myofibroblast cells. This action establishes scar formation and enhances wound strength and takes more than a year.8 Ideally, by the end of the wound healing process, the scar will form with a faint, fine skin-colored scar line without any other symptoms. Especially during the last remodeling phase, if anything goes wrong during the wound healing process, the wound may heal abnormally with pathological scarring.9
Certain risk factors contribute to particular people developing abnormal scars. The size and depth of the scar as well as the direction are intuitive factors. Anatomical location of the wound is also a risk factor. The shoulders, anterior chest, lower abdomen, and skin over bony prominences, as well as other locations with little blood supply, scar poorly.10 Personal and family history of scars, age, and skin tone are other factors that contribute to the scar formation.10 Medication being taken can also interfere with the wound healing process. The doctor should be informed of any of the above-mentioned known risk factors before surgery or procedure so that prophylactic treatment can be assigned before the scar itself needs to be treated.
Hypertrophic
In surgical hypertrophic scars, the cause of the scar is the surgery itself. Specifically, traumas to the lower deep dermis layers in areas where the skin is tighter or there is additional muscle tissue are most susceptible to the development of hypertrophic scars. Adverse healing factors such as infection, excess tension, and repeat traumas are associated with hypertrophic scars.11 Hypertrophic scars form in the presence of elevated levels of TGF-β. Their characteristic elevated, uneven appearance is due to the body producing new collagen fibers at a rate that exceeds the destruction of old collagen.11 In this case, the proportion of type III to type I collagen in the scar is higher than in normal skin. The accumulation of excess collagen results in the raised hypertrophic scar.11
Keloids
Keloids form by the random organization of type III collagen fibers in a dense connective tissue matrix. This ratio of type III to normal collagen is higher in keloid scars than in other scars.11 This is contrary to normal scars that feature collagen bundles arranged parallel to the skin surface. Keloids are ischemic as compared with adjacent normal tissue. It is thought that the greater expression of hypoxia-induced factor-1α and a marked decrease in vascular density contribute to this nature. Research suggests that fibroblasts and myofibroblasts are responsible for the increased deposition of collagen.11 This is indicated by the increased levels of fibronectin produced by fibroblasts. Other theories show keloid formation as stimulated by an allergic, hormone-stimulated, or hypoxia-induced response. Recent studies report keloids as a product of insulin-like growth factors. Scientists generally believe genetic factors impact keloid formation, as certain populations and families form keloids more often (see also chapter 8.2).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


