Hidradenitis suppurativa is difficult to treat owing to its complex pathomechanism; beside the extensive inflammation with abscesses and inflammatory nodules, there is also an architectural loss with sinus tract formation and in severe cases with extensive scarring. Therefore, surgery is mandatory in moderate and severe HS.
Key points
- •
At least in higher stages of hidradenitis suppurativa (HS), surgery should be introduced early after setting the diagnosis.
- •
Preoperatively, immunosuppressive and/or antibacterial medical treatment to calm active inflammation must be considered. Imaging (ultrasonography, MRI) may be helpful.
- •
Depending on the extent and severity of the disease local, tumescent, spinal, and/or general anesthesia are used.
- •
Acute phase surgical treatment and treatment of the chronic continue intermediary phase should be distinguished. Incision and drainage can offer pain relief from a tense fluctuating acute abscess.
- •
After wide excision, different wound closure techniques can be chosen. Secondary intention healing usually ensures good functional/cosmetic results in defects up to 140 cm 2 .
- •
Deroofing, ‘skin-tissue-saving excision with electrosurgical peeling’ (STEEP) and wide excision are preferred surgical methods for the chronic phase.
Introduction
Hidradenitis suppurativa (HS) is difficult to treat owing to its complex pathomechanism; beside the extensive inflammation with abscesses and inflammatory nodules, there is also sinus tract formation and in severe cases extensive scarring. Surgery should be introduced early in the management of HS. Unfortunately, surgical treatment is often performed many years after the initial symptoms of the disease, after numerous ineffective cycles of pharmacotherapy. Such delays are often caused by misdiagnosis, a doctor’s lack of knowledge about the disease, unjustified confidence in the efficacy of noninvasive therapies, anxiety about surgical treatment and the embarrassing location. The tolerance to and satisfaction with, sometimes debilitating, surgical procedures is surprisingly high and may result from the large psychosocial impact of HS. Because the magnitude of life impairment in HS is far greater than in other dermatoses, patients are highly willing to change the condition.
Introduction
Hidradenitis suppurativa (HS) is difficult to treat owing to its complex pathomechanism; beside the extensive inflammation with abscesses and inflammatory nodules, there is also sinus tract formation and in severe cases extensive scarring. Surgery should be introduced early in the management of HS. Unfortunately, surgical treatment is often performed many years after the initial symptoms of the disease, after numerous ineffective cycles of pharmacotherapy. Such delays are often caused by misdiagnosis, a doctor’s lack of knowledge about the disease, unjustified confidence in the efficacy of noninvasive therapies, anxiety about surgical treatment and the embarrassing location. The tolerance to and satisfaction with, sometimes debilitating, surgical procedures is surprisingly high and may result from the large psychosocial impact of HS. Because the magnitude of life impairment in HS is far greater than in other dermatoses, patients are highly willing to change the condition.
Treatment goals and planned outcomes
The comparison of different operative methods of HS is difficult because of the many types of surgery, interindividual differences between patients and between operators, the shortage of randomized trials, and the lack of consensus about the endpoints used. To be able to compare different surgical interventions, clear definitions of outcomes should be defined. We therefore suggest outcomes for future studies.
Relapse Rates
Relapse (owing to nonradical surgery) is defined as inflammatory activity occurring within 0.5 cm of the surgical scar. The natural progression of HS can be defined as inflammation that develops outside this area but in the same anatomic region.
Time to Wound Closure
The time to wound closure is defined as the duration of the wound healing (complete healing) measured in days. For sutured lesions, complete healing may be considered achieved when stitches have been removed.
Complications
Early complications include hemorrhage, infection, hypergranulation, necrosis of grafts or flaps, injury of brachial plexus or big axillary vessels, and thrombosis of brachial veins. Late complications include wound dehiscence, retention of serum (seroma), cicatricial contracture, hypertrophic scars, and keloids.
Patient-Reported Outcomes
Patient satisfaction can be cosmetic or functional. The rate of either is measured on a numerical rating scale of 1 to 10, where 1 corresponds with very dissatisfied and 10 with excellent. If the satisfaction rate is measured for both functional and cosmetic results, the mean rate is shown. The recommendation of the treatment to other people and willingness to undergo further surgery are also important patient-reported outcomes.
Preoperative planning and preparation
Medication to Calm the Inflammation
In moderate and severe HS, it is broadly recommended and accepted that surgery is combined with immunomodulating treatment. However, it remains unclear whether relapse rates after surgery with perioperative immunomodulation therapy are lower than surgical treatments without perioperative medication.
Imaging
Imaging is not used routinely in surgery for HS, although it may be beneficial to management. Some studies with ultrasonography showed that the inflammation can be extended horizontally and vertically far over the visible borders of the inflammation on the skin surface. Moreover, differentiating between enterocutaneous fistula formation in Crohn’s disease remains challenging, especially in the perianal region. Perianal lesions of Crohn’s disease usually present as wide fistulas, entering deeply through the perianal area to the colon and/or vagina, affecting the skin and subcutaneous tissue only to a small extent. Lesions of HS present as purulent, inflammatory infiltrates, frequently reaching the buttocks and perineum with numerous narrow, less visible shallow fistulas reaching the anus. Moreover, mixed clinical presentations can occur because of coexistence of HS and Crohn’s disease.
In ambiguous cases, imaging with ultrasonography, MRI, CT, and fistulography are helpful to assess the location and depth of fistulas and sinuses. Shallow lesions expressing the features of HS can be treated surgically by a (dermato)surgeon, independent from the established diagnosis of Crohn’s disease. If the diagnosis of Crohn’s disease with deep fistulas is confirmed, the surgical treatment should be carried out in cooperation with proctologic specialists. The diagnostic imaging, primarily fistulography, may be decisive.
Procedural approach
Anesthesia
Local anesthesia
Local anesthesia is performed in 2 steps. First, field block anesthesia is performed with lidocaine 1% (10 mg/mL) plus adrenaline (5 μg/mL). Second, nodules and/or sinus tracts are injected with the same local anesthetic. If patients have a fear of needles or if they experience a lot of pain during local anesthesia, lidocaine and prilocaine cream (eutectic mixture of local anesthetics [EMLA]) can be applied 1 hour before the injections.
Tumescent local anesthesia
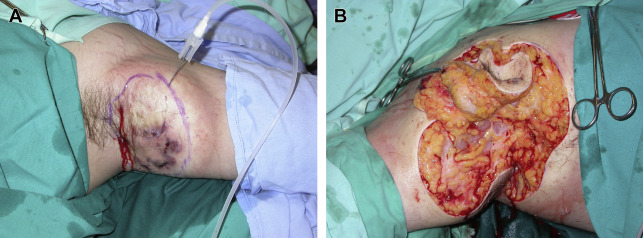
In tumescent local anesthesia (TLA), large volumes (≥100 mL) of highly diluted local anesthetics (usually lidocaine buffered with sodium bicarbonate) are injected subdermally with mechanical assistance. In simple cases, it may be used as the sole method of anesthesia; in more advanced cases, it can be combined with sedation, spinal, or general anesthesia. Because of the necessity of large skin incisions and difficulty in diffusion in indurated, fibrotic tissue, the concentration of lidocaine should be relatively high (0.1%), especially when TLA is used as the sole form of anesthesia. If TLA is used as a complementary agent, the concentration of lidocaine may be as low as 0.04% to 0.05%. Because the absorption of lidocaine is expected to be relatively high in lesional HS tissue, a maximal dose of 35 mg/kg lidocaine is recommended. The concentration of other components of TLA solution are as usual: adrenaline (1:1–2 million) and sodium bicarbonate (10–20 mL in 1000 mL 0.9% NaCl). The tumescent solution is injected abundantly with use of a rotation pump, special tubing, and long (spinal) needles. Owing to specific properties of TLA, intraoperative and postoperative bleeding is greatly reduced, ensuring accurate and safe surgery and minimal blood loss, and the risk of infection is diminished owing to antiseptic activity of bicarbonate and the wash away of infectious agents by copious discharge of fluid from the wound. Finally, postoperative pain is decreased for many hours ( Fig. 1 ).
General and spinal anesthesia
Under general and spinal anesthesia, large areas can be operated on without the limitation of the maximum allowed amount of local anesthetics. In addition, some patients favor general anesthesia above local anesthesia, which can be painful and difficult to achieve in areas of active inflammation and fibrosis.
Lesion Removal Techniques
Incision and drainage
The purpose of incision and drainage is pain relief in case of a tense, fluctuating acute abscess. There is only a short-term effect, because lesions treated by incision and drainage tend to relapse. For drainage, 6- to 8-mm punch biopsies can be used. By digital pressure and rinsing with saline solution, the remaining pus is removed.
Deroofing
The deroofing technique was first described by Mullins and colleagues in 1959. In the 1980s, the technique was modified by preservation of the exposed lesion floor. Presently, there is a tendency to remove keratinous debris and viable epithelial remnants on the floor because these substances could cause relapses when left present. Deroofing is the primary surgical therapy for persisting nodules or sinus tracts in HS Hurley stage I/II. The procedure starts with identification of the HS lesions to be deroofed by physical examination. Local anesthesia is performed as described under Medication to Calm the Inflammation and Imaging. Next, a blunt probe is used to identify sinus openings. After introduction, the probe is placed at different angels in search of connecting fistulas. The probe should be inserted into the fistula without resistance. If force is applied, false tracts can be created with the probe. The sinus roof is removed using electrosurgical dissection with a wire loop tip coupled to an electrosurgical generator ( Fig. 2 ). The probe is used as a guide, leaving the epithelial bottom of the sinus tract intact. The margins must be probed again for residual communicating sinus tracts. The jellylike material on the floor of the sinus tract needs to be removed superficially with the wire loop tip. The defects are left open for healing by secondary intention.
Skin-tissue–saving excision with electrosurgical peeling
This surgical technique for HS was described by Blok and colleagues : the skin-tissue–saving excision with electrosurgical peeling (STEEP) procedure. STEEP seems to be a promising alternative to wide excision in extensive disease because it saves healthy tissue to a maximum and achieves complete removal of lesional tissue ( Fig. 3 ). The idea is that tissue sparing leads to quick wound healing, good cosmetic results, and low risk of contractures. Recurrence rates seem similar to wide excision because both techniques are aimed at complete removal of lesional and fibrotic tissue. STEEP is performed mostly under general anesthesia. Preoperatively, the operation field is palpated and sinus tracts are probed to get an impression about the extent of the disease. Next, the sinus roofs are incised electrosurgically with a wire loop tip coupled to an electrosurgical generator. Subsequently, successive tangential excisions are made until the epithelialized floor of the sinus tract is reached. Tangential peeling off affected tissue is continued until the area is clear of lesional tissue and fibrosis. Thereafter, the wound edges are checked with a probe for remaining sinus tracts. During and after the procedure, hemostasis is achieved by using the coagulation mode of the Erbotoom. Finally, the margins of the wound can be injected with triamcinolonacetonide 10 to 20 mg to prevent hypergranulation and bupivacaine 0.5% (10 mL) for postoperative analgesia. The defects are left open for healing by secondary intention ( Fig. 4 ).
Excision
Excision is aimed at complete removal of lesions. The extent of pathologic lesions should be determined by observation in bright illumination and palpation showing the leakage of pus after compression. Furthermore symptoms reported by the patient should be taken into consideration, like localized pain and drainage.
Different surgical approaches are used with varying degrees of invasiveness. In limited local excision, each separate lesion is excised with a certain margin of healthy tissue. In wide excision, an area embracing all lesions is removed. In radical excision, an entire area of a body region in which the disease may presumable spread is excised. For all 3 techniques, often a lateral margin of 1 cm is proposed. However, in small lesions, to ensure complete removal, a sparse margin may be sufficient. There is no consensus about whether partial or complete removal of the subcutaneous fat should be achieved. It is advised to adjust the excision to the extent and severity of the disease, as well as to the dynamics of its development. Particularly at depth, in proximity of big neurovascular bundles in axillary and inguinal regions, as well as around the rectum, overzealous excisions should be avoided. The complications of such interventions may cause more morbidity than the disease itself ( Fig. 5 ). That is why recommendation for curettage of any remaining walls of sinuses is given, instead of thorough excision in these cases ( Fig. 6 ).
Wound Closure Techniques
Primary closure
Sutures
Simple sutures may be recommended in small defects surrounded by loose skin. Undermining as well as suturing under high tension should be avoided, because of risk of healing disturbances. This option usually ensures fast healing with good cosmetic and functional results ( Fig. 7 ). It is advisable to close the wound rather loosely, which enables the outflow of exudate and limits risk of infection.
Split-thickness skin grafts
Split-thickness skin grafts, usually meshed, are used typically in large wounds. Grafts of 0.6 to 0.8 mm thickness are harvested from the thighs or buttocks with use of dermatomes, and then they are expanded in a ratio of 3:1 by multiple incisions in the mesh graft device. Grafts allow for closure of even the largest wounds with minimal risk of serious complications. Despite evident differences of color and texture with surrounding skin, they ensure acceptable functional and aesthetic results, especially in the armpits and buttocks ( Fig. 8 ). Traditionally, skin grafts were put on granulation tissue, after longer period of wound conditioning. Owing to good hemostatic properties, TLA grafting can also be performed in 1 procedure, directly after excision. Only on genital and inguinal regions is skin grafting made on previously granulated wound bed because of the high risk of infection. Morgan and colleagues compared split skin grafting and secondary intention healing (SIH) in 10 patients undergoing bilateral excision for axillary HS. In each patient, 1 axilla was grafted and the other was allowed for SIH using a Silastic foam dressing. Split skin grafting had a shorter time to wound closure than SIH. However, a majority of patients preferred SIH because of the comfort during healing, limb freedom, and lack of a painful donor site. Additionally, SIH leads to good cosmetic results, whereas skin grafting often gives a patchwork appearance with a persistent depression at the site of excision.
Related posts:
 Prevalence, Risk Factors, and Comorbidities of Hidradenitis Suppurativa
Diagnosing Hidradenitis Suppurativa
Prevalence, Risk Factors, and Comorbidities of Hidradenitis Suppurativa
Diagnosing Hidradenitis Suppurativa
 The Handicap of Hidradenitis Suppurativa
Endocrinologic Aspects of Hidradenitis Suppurativa
Inflammatory Mechanisms in Hidradenitis Suppurativa
The Handicap of Hidradenitis Suppurativa
Endocrinologic Aspects of Hidradenitis Suppurativa
Inflammatory Mechanisms in Hidradenitis Suppurativa
 Randomized Controlled Trials for the Treatment of Hidradenitis Suppurativa
Randomized Controlled Trials for the Treatment of Hidradenitis Suppurativa
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


