Hidradenitis suppurativa (HS) is a chronic, inflammatory, recurrent, debilitating skin disease. Several treatment modalities are available, but most of them lack high-quality evidence. A systematic search was performed to identify all randomized controlled trials for the treatment of HS in order to review and evaluate the evidence. Recommendations for future randomized controlled trials include using validated scores, inclusion of patient rated outcomes, and thorough report of side effects. Evidence for long-term treatment and benefit/risk ratio of available treatment modalities is needed in order to enhance evidence-based treatment in daily clinical practice. Combining surgery with antiinflammatory treatment warrants further investigation.
Key points
- •
Hidradenitis suppurativa (HS) is a chronic debilitating skin disease.
- •
High-quality evidence for the different treatment modalities of HS is lacking.
- •
Eleven randomized controlled trials are available concerning the treatment of HS.
- •
A variety of outcome parameters has been used, preventing indirect comparison.
- •
The need for appropriately designed randomized controlled trials is emphasized.
Introduction
Hidradenitis suppurativa (HS) is a chronic, inflammatory, recurrent, scarring, debilitating skin disease that usually presents after puberty. HS also inflicts a significant burden on patients. Epidemiologic studies also highlight that patients with HS present several cardiovascular risk factors, such as smoking, obesity, dyslipidemia (low high-density lipoprotein levels and hypertriglyceridemia), diabetes, and metabolic syndrome, at a significantly higher rate compared with healthy controls. This evidence indicates that HS is more than a disease limited to skin and that it displays systemic chronic inflammation characteristics, like psoriasis.
In the evaluation of trials and reported treatment results, disease quantification is of the outmost importance. Hurley stage ( Table 1 ), Modified Sartorius Score (MSS), and HS Physician’s Global Assessment (HS-PGA) ( Table 2 ) are measures that have been used to classify and assess HS disease severity ( Box 1 ). A new score was recently developed, evaluated, and validated as a clinical outcome for assessment of treatment effectiveness, especially for the inflammatory manifestations: the Hidradenitis Suppurativa Clinical Response (HiSCR). The use of this validated, easy-to-use score is recommended in both research and daily clinical practice and it allows easier comparisons when assessing different trials. At present the inconsistencies in reported outcomes make such comparisons difficult.
| Hurley Stage | Definition |
|---|---|
| I | Abscess formation, single or multiple, without sinus tracts and cicatrization |
| II | Single or multiple, widely separated, recurrent abscesses with tract formation and cicatrization |
| III | Diffuse or near-diffuse involvement, or multiple interconnected tracts and abscesses across the entire area |
| Clear (score = 0) | 0 abscesses, 0 draining fistulas, 0 inflammatory nodules, and 0 noninflammatory nodules |
| Minimal (score = 1) | 0 abscesses, 0 draining fistulas, 0 inflammatory nodules, and presence of noninflammatory nodules |
| Mild (score = 2) | 0 abscesses, 0 draining fistulas, and 1–4 inflammatory nodules; or 1 abscess or draining fistula and 0 inflammatory nodules |
| Moderate (score = 3) | 0 abscesses, 0 draining fistulas, and ≥5 inflammatory nodules; or 1 abscess or draining fistula and ≥1 inflammatory nodule; or 2–5 abscesses or draining fistulas and <10 inflammatory nodules |
| Severe (score = 4) | 2–5 abscesses or draining fistulas and ≥10 inflammatory nodules |
| Very severe (score = 5) | >5 abscesses or draining fistulas |
Classification/severity assessment:
- •
Hurley stage
- •
MSS
- •
HS-PGA
Treatment effectiveness assessment:
- •
HiSCR (inflammatory manifestations)
- •
Inflammatory nodules, abscesses, and draining fistulas count
Comorbidities assessment:
- •
Quality of life (DLQI)
- •
Pain (VAS)
- •
Smoking
- •
Obesity (BMI, WC)
- •
Metabolic syndrome (NCEP-ATP III)
- •
Diabetes
- •
Anemia
- •
Dyslipidemia
- •
Work productivity (WPAI)
Abbreviations: BMI, body mass index; DLQI, Dermatology Life Quality Index; HiSCR, hidradenitis suppurativa clinical response; NCEP-ATP III, national cholesterol education program adult treatment panel III criteria; VAS, visual analog scale; WC, waist circumference; WPAI, work productivity and activity impairment questionnaire.
A variety of treatment methods are available for HS, but only a few of them are based on high-quality evidence. This article gives an overview of the currently available evidence for the pharmacologic as well as invasive treatment modalities of HS to facilitate rational decision making in daily clinical practice and elucidate recommendations for future randomized clinical trials.
Introduction
Hidradenitis suppurativa (HS) is a chronic, inflammatory, recurrent, scarring, debilitating skin disease that usually presents after puberty. HS also inflicts a significant burden on patients. Epidemiologic studies also highlight that patients with HS present several cardiovascular risk factors, such as smoking, obesity, dyslipidemia (low high-density lipoprotein levels and hypertriglyceridemia), diabetes, and metabolic syndrome, at a significantly higher rate compared with healthy controls. This evidence indicates that HS is more than a disease limited to skin and that it displays systemic chronic inflammation characteristics, like psoriasis.
In the evaluation of trials and reported treatment results, disease quantification is of the outmost importance. Hurley stage ( Table 1 ), Modified Sartorius Score (MSS), and HS Physician’s Global Assessment (HS-PGA) ( Table 2 ) are measures that have been used to classify and assess HS disease severity ( Box 1 ). A new score was recently developed, evaluated, and validated as a clinical outcome for assessment of treatment effectiveness, especially for the inflammatory manifestations: the Hidradenitis Suppurativa Clinical Response (HiSCR). The use of this validated, easy-to-use score is recommended in both research and daily clinical practice and it allows easier comparisons when assessing different trials. At present the inconsistencies in reported outcomes make such comparisons difficult.
| Hurley Stage | Definition |
|---|---|
| I | Abscess formation, single or multiple, without sinus tracts and cicatrization |
| II | Single or multiple, widely separated, recurrent abscesses with tract formation and cicatrization |
| III | Diffuse or near-diffuse involvement, or multiple interconnected tracts and abscesses across the entire area |
| Clear (score = 0) | 0 abscesses, 0 draining fistulas, 0 inflammatory nodules, and 0 noninflammatory nodules |
| Minimal (score = 1) | 0 abscesses, 0 draining fistulas, 0 inflammatory nodules, and presence of noninflammatory nodules |
| Mild (score = 2) | 0 abscesses, 0 draining fistulas, and 1–4 inflammatory nodules; or 1 abscess or draining fistula and 0 inflammatory nodules |
| Moderate (score = 3) | 0 abscesses, 0 draining fistulas, and ≥5 inflammatory nodules; or 1 abscess or draining fistula and ≥1 inflammatory nodule; or 2–5 abscesses or draining fistulas and <10 inflammatory nodules |
| Severe (score = 4) | 2–5 abscesses or draining fistulas and ≥10 inflammatory nodules |
| Very severe (score = 5) | >5 abscesses or draining fistulas |
Classification/severity assessment:
- •
Hurley stage
- •
MSS
- •
HS-PGA
Treatment effectiveness assessment:
- •
HiSCR (inflammatory manifestations)
- •
Inflammatory nodules, abscesses, and draining fistulas count
Comorbidities assessment:
- •
Quality of life (DLQI)
- •
Pain (VAS)
- •
Smoking
- •
Obesity (BMI, WC)
- •
Metabolic syndrome (NCEP-ATP III)
- •
Diabetes
- •
Anemia
- •
Dyslipidemia
- •
Work productivity (WPAI)
Abbreviations: BMI, body mass index; DLQI, Dermatology Life Quality Index; HiSCR, hidradenitis suppurativa clinical response; NCEP-ATP III, national cholesterol education program adult treatment panel III criteria; VAS, visual analog scale; WC, waist circumference; WPAI, work productivity and activity impairment questionnaire.
A variety of treatment methods are available for HS, but only a few of them are based on high-quality evidence. This article gives an overview of the currently available evidence for the pharmacologic as well as invasive treatment modalities of HS to facilitate rational decision making in daily clinical practice and elucidate recommendations for future randomized clinical trials.
Methodology
In order to objectively identify all randomized controlled clinical trials (RCTs) for the treatment of HS, a systematic search was undertaken in the electronic databases MEDLINE, EMBASE, and CENTRAL up to January 30 2015, using a draft search strategy for RCTs for MEDLINE (OVID), as suggested in the Cochrane Handbook. Eligible criteria were RCTs that included patients with HS. Study designs other than RCTs were excluded. Conference abstracts and review articles were also excluded. There was a restriction for the English language. Information from each study was extracted using a standardized data extraction form. To assess the methodological quality, the Risk-of-bias tool suggested in the Cochrane Handbook for Systematic Reviews of Interventions was used. The following items were critically appraised and extracted: method of generation of the randomization sequence, allocation concealment, blinding of participants, researchers and outcome assessors, incomplete outcome data (attrition bias), and selective reporting (reporting bias). In addition, the baseline characteristics of study groups were checked for confounding factors in order to rule out selection bias.
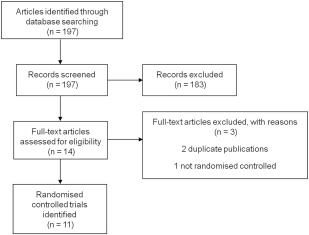
Results
The systematic search provided 197 results. After screening, 11 studies met the inclusion criteria. The selection process is summarized in Fig. 1 . General study characteristics are summarized in Table 3 and the most important results in Table 4 . Four studies involved biologic therapy with anti–tumor necrosis factor (TNF) alpha. Two studies investigated the role of antibiotics, and 1 study investigated hormonal therapy. Also, 3 studies on laser treatment and 1 study of surgical treatment were included. The methodological quality of all studies is separately presented in Fig. 2 and pooled in a graph in Fig. 3 .
| Citation | Setting | Methods | Patients | Intervention Groups | Control Group | Limitations |
|---|---|---|---|---|---|---|
| Clemmensen, 1983 | Denmark | Single-center, double-blind, placebo-controlled trial | 30 patients with HS Hurley I and mild Hurley II | 13 Topical CL 1% (dosing schedule unknown) for 12 wk | 14 PL for 12 wk | Unjustifiable sample size, no intention-to-treat analysis |
| Mortimer et al, 1986 | United Kingdom | Single-center, double-blind, controlled, crossover trial | 24 F patients with HS with moderate to severe HS | 10 oral ethinyl estradiol 50 μg/CPA 50 mg (each menstrual cycle) for 12 mo (with crossover at 6 mo) | 8 oral ethinyl estradiol 50 μg/norgestrel 500 μg (each menstrual cycle) for 12 mo (with crossover at 6 mo) | Unjustifiable sample size, no intention-to-treat analysis |
| Jemec & Wendelboe, 1998 | Denmark | Single-center, randomized, double-blind, controlled trial | 46 patients with HS (39 F, 7 M), Hurley I and II | 16 (13 F, 3 M) oral TCN 500 mg bid plus topical PL, minimum of 3 mo | 18 (15 F, 3 M) topical CL 1% bid plus oral PL, minimum of 3 mo | Unjustifiable sample size, no intention-to-treat analysis |
| Buimer et al, 2008 | Netherlands | Single-center, randomized, controlled trial | 200 patients with HS | 124 (108 F, 16 M) surgical excision with PC plus GC | 76 (72 F, 4 M) surgical excision with PC alone | No clear assessment of baseline severity |
| Mahmoud et al, 2010 | United States | Single-center, randomized, controlled split-body trial | 22 patients with HS (19 F, 3 M), Hurley II | Nd:YAG laser monthly for 4 mo plus BP wash 10% and CL 1% lotion | BP wash 10% and CL 1% lotion alone | No clear report on side effects |
| Adams et al, 2010 | United States | Single-center, randomized, double-blind, placebo-controlled trial | 20 patients with HS with moderate to severe HS | 10 (6 F, 4 M), ETA SC 50 mg twice/wk for 12 wk | 10 (7 F, 3 M), PL SC 50 mg twice/wk for 12 wk | Unjustifiable sample size |
| Grant et al, 2010 | United States | Single-center, randomized, double-blind, placebo-controlled, crossover trial | 38 patients with HS with moderate to severe HS | 15 (12 F, 3 M) IFX (5 mg/kg) IV on wk 0, 2, and 6 | 23 (14 F, 9 M) PL (5 mg/kg) IV on wk 0, 2, and 6 (with crossover at 8 wk) | — |
| Highton et al, 2011 | United Kingdom | Single-center, randomized, controlled split-body trial | 18 HS (15 F, 3 M) patients, Hurley II and III | IPL twice/wk for 4 wk | No treatment | Unjustifiable sample size, no clear report on side effects |
| Miller et al, 2011 | Denmark | Two-center, randomized, double-blind, placebo-controlled trial | 21 patients with HS with moderate to severe HS | 15 (12 F, 3 M) ADA SC 80 mg at baseline, 40 mg eow for 12 wk | 6 (5 F, 1 M) PL SC 80 mg at baseline, 40 mg eow for 12 wk | Early termination of recruitment, difference in baseline severity |
| Kimball et al, 2012 | United States, Denmark, Netherlands, Germany | Multicenter, randomized, double-blind, placebo-controlled trial | 154 patients with HS with moderate to severe HS | 51 (36 F, 15 M) ADA SC 160 mg wk 0, 80 mg wk 2, 40 mg weekly for 16 wk 52 (38 F, 14 M) ADA SC 80 mg wk 0, 40 mg eow for 16 wk | 51 (36 F, 15 M) PL for 16 wk | — |
| Fadel & Tawfik, 2015 | Egypt | Single-center, randomized, controlled, split-body trial | 10 patients with HS (7 F, 3 M) 4 Hurley I, 4 Hurley II, 2 Hurley III | NMB gel plus IPL, twice monthly, maximum 6 mo | Free NMB gel plus IPL, twice monthly, maximum of 6 mo | Unjustifiable sample size |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


