It is challenging to estimate a true prevalence of hidradenitis suppurativa (HS) because it is underdiagnosed and misdiagnosed. Prevalences have been reported from 0.00033% to 4.1%. The incidence seems to be rising. In addition to dermatologic symptoms, HS is associated with metabolic syndrome, and increased cardiovascular risk. The majority of HS patients are smokers. Additional somatic comorbidities complicating HS include autoimmune conditions, follicular syndromes, rheumatologic conditions, and malignancies. HS patients are troubled by psychological comorbidities. When treating HS patients it is imperative not only to treat the skin symptoms, but also address the screening and treatment of possible comorbidities.
Key points
- •
The true prevalence of hidradenitis suppurativa (HS) is challenging to estimate because it is often under diagnosed and misdiagnosed; the incidence seems to be increasing.
- •
HS is associated with a wide range of somatic comorbidities, from metabolic syndrome to rheumatologic conditions, as well as psychological comorbidities.
- •
The sum of somatic and psychological comorbidities places significant burden on HS patients beyond dermatologic symptoms.
- •
Treatment of HS needs to target dermatologic symptoms as well as possible comorbidities.
Prevalence and incidence
As hidradenitis suppurativa (HS) has been an orphan disease for decades and subsequently a highly misdianogsed and underdiagnosed condition with a significant diagnose delay, the true prevalence has been correspondingly challenging to estimate. Prevalences are reported as low as 0.00033% and as high as 4.1%.
Prevalence estimates seem to fluctuate according to the nature of the study design, participants, and geography. A uniform pattern based on these methodologic differences present low prevalence rates in predominantly American studies performed on insurance databases, and contrasting higher prevalences in studies based on an HS diagnosis determined by physical examination or interviews/questionnaires.
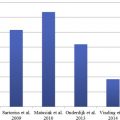
In a health-insured–only US population of 15,054,519 participants, Cosmatos and colleagues found an unadjusted prevalence of 0.053%. A similar low prevalence was found in the Massachusetts General Hospital Database.
In contrast, a Danish study based on HS symptomatology in 100 females from the staff or patients referred to Department of Dermatology reported a prevalence of 4%. A similar point prevalence of 4.1% was described in Danish study based on physical examination of 507 patients undergoing screening for sexually transmitted diseases.
Questionnaires aimed at diagnosing HS using simple descriptions of symptoms, for example, boils and location of the boils, suggest a specificity and sensitivity of 82% to 97% and 90% to 97%, respectively. A French population-based questionnaire study of 10,000 participants found a prevalence of 1%, and a more recent Danish population study of 17,454 participants from the general population reported a prevalence of 2.1%.
The incidence of HS based on an American database has been suggested to be 6 per 100,000 person-years, and seem to be increasing. Thus, an increase from 4.3 per 100,000 (during 1970–1979) to 9.6 per 100,000 (during 2000–2008) was noted.
Prevalence and incidence
As hidradenitis suppurativa (HS) has been an orphan disease for decades and subsequently a highly misdianogsed and underdiagnosed condition with a significant diagnose delay, the true prevalence has been correspondingly challenging to estimate. Prevalences are reported as low as 0.00033% and as high as 4.1%.
Prevalence estimates seem to fluctuate according to the nature of the study design, participants, and geography. A uniform pattern based on these methodologic differences present low prevalence rates in predominantly American studies performed on insurance databases, and contrasting higher prevalences in studies based on an HS diagnosis determined by physical examination or interviews/questionnaires.
In a health-insured–only US population of 15,054,519 participants, Cosmatos and colleagues found an unadjusted prevalence of 0.053%. A similar low prevalence was found in the Massachusetts General Hospital Database.
In contrast, a Danish study based on HS symptomatology in 100 females from the staff or patients referred to Department of Dermatology reported a prevalence of 4%. A similar point prevalence of 4.1% was described in Danish study based on physical examination of 507 patients undergoing screening for sexually transmitted diseases.
Questionnaires aimed at diagnosing HS using simple descriptions of symptoms, for example, boils and location of the boils, suggest a specificity and sensitivity of 82% to 97% and 90% to 97%, respectively. A French population-based questionnaire study of 10,000 participants found a prevalence of 1%, and a more recent Danish population study of 17,454 participants from the general population reported a prevalence of 2.1%.
The incidence of HS based on an American database has been suggested to be 6 per 100,000 person-years, and seem to be increasing. Thus, an increase from 4.3 per 100,000 (during 1970–1979) to 9.6 per 100,000 (during 2000–2008) was noted.
Risk factors and comorbidities
There is a considerable overlap between what are characterized risk factors and comorbidities. One possible definition of a risk factor is something that increases a person’s chances of developing a disease, whereas a comorbidity may be defined as a coexisting medical condition or disease process, and may be categorized as psychological or somatic.
Age and Sex
The mean age of onset is the early 20s; however, HS has additionally been reported children and postmenopausal women. Considerable literature state a decline in prevalence after the age of 55, which may reflect an age-related clinical burnout of the HS activity or hormonal changes. Equivalently, the observation that the female:male ratio is 3:1 led to the theory of androgens playing a pathogenetic part in HS. However, investigations have failed to support this hypothesis.
Obesity
A sizable body of literature demonstrates obesity as a paramount risk factor. Recently, a cross-sectional hospital- and population-based study comparing 32 hospital-based HS subjects, 326 population-based HS subjects, and 14,851 controls (non-HS subjects) found an odds ratio (OR) for obesity (body mass index [BMI] ≥30 kg/m 2 ) of 6.38 (95% CI, 2.99–13.62) and 2.56 (95% CI, 2.00–3.28) for hospital- and population-based HS subjects, respectively, when compared with controls. Correspondingly, this study found an OR for abdominal obesity of 3.62 (95% CI, 1.73–7.60) and 2.24 (95% CI, 1.78–2.82) for the hospital- and population-based HS subjects, respectively. Additionally, 2 studies including 336 and 80 hospital-based HS patients compared with controls found an association of HS and BMI as well as abdominal obesity. Ambiguous results have, however, been described.
An association between BMI and the HS severity measurement Sartorius score was found in 251 HS patients implying a dose–response relationship. Moreover, the higher OR reported for hospital HS subjects compared with HS subjects from the general population might reflect differences in HS severity, and therefore be supportive of the dose–response relationship. Nonetheless, results remain inconsistent with regard to severity, and surprisingly some studies have reported no correlation between the severity or duration of HS and obesity.
Interventional studies are limited. However, 1 study demonstrated that a weight reduction of 15% in patients with BMI of greater than 30 kg/m 2 ameliorates HS supporting a dose–response relationship. Moreover, obesity was reported as a risk factor for recurrence after CO 2 laser treatment of HS patients.
Some factors may aid the pathophysiologic mechanisms behind the association of obesity and HS. The adipose cells are considered an independent endocrine tissue capable of secreting proinflammatory cytokines, which may add to the chronic inflammatory state of HS. Furthermore, obesity may lead to large skin folds enhancing the warm, humid milieu and skin-to-skin contact making a mechanically dependent exacerbation or maintenance of the HS lesions.
Smoking
Various studies report an association between smoking and HS. Rates of smoking in HS patients have been noted from 42% up to 70% to 92%. A German study found the odds of having HS to be 9.4 times greater in current smokers versus non/ex-smokers. Additionally, a French population-based study described a link between HS and current smoking, but not prior smoking. The association with smoking has also been related to clinical HS disease severity. It has recently been proposed that nonsmoking and nonobesity is associated with a better chance of HS remission, and it has come to light that HS surgery combined with smoking cessation give rise to fewer or no lesions. Further aiding the dose–response relationship is a study investigating the role of smoking and obesity concluding that the severity of HS is worse in previous smokers when compared with never-smokers.
A relationship between cigarette smoking and inflammation has been established previously. Kurzen and colleagues hypothesized on possible pathophysiologic mechanisms of smoking on HS, for example, modification in the microflora of the skin and a prolonged secretion of nicotine in sweat inducing tumor necrosis factor (TNF)-α release and follicular occlusion.
Genetics
There also seems to be a genetic component to HS, which is discussed in greater detail by Ingram . Briefly, in 1985 Fitzsimmons and colleagues identified a strong family predisposition with 34% of patient relatives having the disease as well. Three subsequent studies have also observed familial associations in HS patients. Through genetic investigations, an autosomal-dominant defect encoding γ-secretase has been linked to rare forms of HS. Additionally, a mutation in the proline–serine–threonine phosphatase-interacting protein 1 (PSTPIP1) gene has been identified in the pyoderma gangrenosum (PG), acne, HS, and pyogenic arthritis (PAPASH) syndrome involving HS. This syndrome is discussed elsewhere in this article. Mutations in this gene have also been implicated in autoinflammatory syndromes. A possible association of HS to HLA-B, HLA-DR, or CARD15 polymorphisms has not been found so far.
Other Risk Factors
Additional risk factors associated with worsening of the HS disease activity are heat, exercise, sweating, stress, fatigue, friction, tight clothing, deodorants, other cosmetics, shaving, menstruation, and brewers yeast. However, the body of evidence concerning these risk factors is limited.
Metabolic Comorbidities
Metabolic comorbidities involves medical conditions of, relating to, or resulting from metabolism, that is, anabolic or catabolic processes. Preceding research of metabolic comorbidities in inflammatory diseases has provided evidence of an association between the metabolic syndrome and, for example, psoriasis, rheumatoid arthritis, and systemic lupus erythematosus.
Increasing evidence furthermore proposes HS to be associated with the metabolic syndrome. Because the metabolic syndrome is a cluster of cardiovascular risk factors including diabetes/insulin resistance, hypertension, dyslipidemia, and obesity, there is a clear overlap between this comorbidity and the risk factors obesity and smoking.
Sabat and colleagues and Gold and colleagues performed hospital-based studies of 80 and 366 HS patients, respectively, and found the metabolic syndrome to be a comorbidity of HS. Gold and colleagues found that 50.6% of HS patients compared with 30.2% of the controls suffered from the metabolic syndrome ( P <.001). Equivalently, Sabat and colleagues reported 40% of HS patients versus 13% of controls having the metabolic syndrome yielding an OR of 4.46 (95% CI, 2.02–9.96). A large Danish study including both a population- and a hospital-based sample of 358 HS subjects confirmed these results, and demonstrated 32.2% of population-based HS subjects and 53.1% of hospital-based HS subjects versus 21.5% of controls with the metabolic syndrome resulting in a higher OR for the hospital-based HS subjects (OR, 3.89 [95% CI, 1.90–7.98] vs OR, 2.08 [95% CI, 1.61–2.69]). Because hospital-based HS subjects may have a more severe degree of HS, these results may advocate a dose–response relationship and, according to Hills causal criteria, this could favor a possible causal relation. Even so, all studies so far have been observational and subsequently cannot prove causality.
Possible pathophysiologic mechanisms behind the supposed association of HS and the metabolic syndrome introduce a hypothesis concerning the long-term effects of the chronic inflammatory state of HS, the sedentary lifestyle (ie, overeating, lack of physical exercise) that may accompany HS patients as a consequence of psychological stigmatization, inflammation-induced neuropsychological factors affecting appetite and cortisone levels, and concomitant pharmacotherapy with subsequent increased cardiovascular risk.
Autoimmune Comorbidities
There is significant overlap between patients with HS and inflammatory bowel disease (IBD), especially Crohn’s disease (CD). A recent cross-sectional study of 1093 patients with IBD found that 255 of these patients (23%) also had HS. More specifically, 26% of those with CD and 18% of ulcerative colitis patients also had HS. Similar findings were reported by these authors in their 2010 evaluation of 158 IBD patients.
Further complicating the matter is the fact that differentiating cutaneous CD from HS may prove difficult. Jemec and colleagues described lesions in CD to be more ulcerative, the scars more retractile, and largely confined to the anorectal skin and initial rectal mucosa. However, these lesions commonly extend to create fistulas, strictures, and even incontinence when the anal sphincter is involved. HS lesions, on the other hand, do not form endoanal lesions or primary ulcerations. Comedones, nodules, skin bridging, and sinuses are present instead. Physical examination should be adequate to distinguish these 2 entities in most cases, but MRI may be useful for some cases of perianal IBD versus HS. It should also be noted that patients can have both HS and IBD. In both IBD studies mentioned, van der Zee and colleagues did not ask about involvement of the perianal area to avoid confusion with cutaneous perianal lesions associated with CD, so these studies may actually underrepresent the number of IBD patients with HS.
One retrospective study of 61 HS cases found 24 patients (38%) also had a diagnosis of CD. On average, the diagnosis of CD predated the diagnosis of HS by 3.5 years. Another study including 37 cases of HS and CD also found the diagnosis of CD usually predated HS, and it was speculated that, because both CD and HS have compromised barriers (cutaneous and intestinal), an abnormal immune response from pathogen exposure or genetics may be involved.
PG is a rare inflammatory condition that commonly presents as a painful nodule on the lower extremity before breaking down to an ulcer with a raised, undermined border. PG has known associations with IBD, inflammatory arthritis, and myeloproliferative disorders. Furthermore, several syndromes with PG and HS have been named: PASH (PG, acne conglobata, and HS), PAPASH (PG, acne, HS, and pyogenic arthritis), and PASS (PG, acne conglobata, HS, and axial spondyloarthopathy).
To date, 33 nonsyndromic cases of PG and HS have been described in the literature. Eleven of these cases were reported in a 2010 multicenter, retrospective study. Interestingly, the onset of HS predated PG in all patients with a mean time of 2.5 years prior. Additionally, the mean onset of HS before PG in 20 cases in the literature before 2010 was found be 19 years. The average age for each disease onset was 24 and 43 years, respectively.
Three PG and HS syndromes are reported in the literature. Each of these syndromes consists of the triad of PG, acne conglobata, and HS, and are be differentiated clinically by their arthritic component: PAPASH (pyogenic arthritis), PASS (seronegative spondyloarthritis), and PASH (no arthritis). Genetically, PASS seems to be a distinct condition with no gene mutations identified. PAPASH and PASH may share a common underlying pathophysiology, because a missense mutation (c.831G→T nucleotide substitution) in the PSTPIP1 gene and increased number of microsatellite repeats in the PSTPIP1 promoter region has been found in each syndrome, respectively. PSTPIP1 gene mutations have also been described in PAPA syndrome (triad of PG, acne conglobata, and pyogenic arthritis) and familial Mediterranean fever (an autoinflammatory disorder).
PSTPIP1 regulates immune activation through its interaction with pyrin. Pyrin downregulates the immune system by decreasing interleukin (IL)-1β production that, in turn, decreases subsequent production and release of several inflammatory cytokines. When mutated, PSTPIP1 seems to exert a dominant-negative effect on pyrin, increasing IL-1β and neutrophil-mediated inflammation. Thus, patients with PASH syndrome have significantly greater expression of cutaneous IL-1β and its receptors I and II ( P = .028, .047, and .050, respectively) compared with controls. Interestingly, PASH’s serum inflammatory markers do not seem to be elevated, indicating that the inflammatory process in PASH is mainly localized in the skin. Reports of patients with PASH treated with the IL-1 receptor antagonist (IL-1RA), anakinra, have shown mixed results. Thus, IL-1RA may only confer partial blockage of IL-1β. Further investigation on the utility of IL-1RA in PASH syndrome is warranted.
In addition to IL-1β, recent findings indicate a possible role of IL-17 in PASH. In Garzorz and colleagues’ report on a patient with PASH and psoriasis, 2 punch biopsies (one consistent with psoriasis, the other with PG) revealed a prominent infiltrate of IL-17–positive immune cells by immunohistochemistry. Following initiation of a TNF-α inhibitor, IL-17 and IL-22 levels were found to be 5 times greater than those of health controls. Although these results could be driven solely by the patient’s psoriasis, the utility of future IL-17 blockers in patients with variants of PASH/PAPASH syndrome should not be excluded.
Follicular Occlusion Triad, Acne, and Syndromes
The basic etiopathogenesis of HS has been partly attributed to follicular occlusion from infundibular hyperkeratosis and follicular epithelium hyperplasia. This occlusion incites perifollicular inflammation and follicular rupture, leading to the formation of the cysts, abscesses, and sinus tracts that define the clinical pathology of HS. In addition to HS, follicular occlusion is an etiologic factor in acne conglobata and dissecting cellulitis of the scalp as well. Kierland first described the concurrence of these 3 conditions in 1951 as the follicular occlusion triad. Shortly thereafter, Brunsting highlighted commonalities between the conditions, including hyperplasia of the pilosebaceous apparatus, follicular occlusion, bacterial invasion with suppuration, and cicatricial healing. In 2013, subtypes for HS were described following Latent Class modeling (LC): LC1 being axillary–mammary, LC2 as follicular, and LC3 as gluteal.
There are several cases in the literature citing the coincidence of follicular occlusion disorders in the same patient. More recently, pilonidal sinuses have been recognized to accompany this group of follicular occlusion disorders, creating the follicular occlusion tetrad: HS, acne conglobata, dissecting cellulitis, and pilonidal cysts.
Acne vulgaris has also been associated with HS. In an American and a French study 36.2% and 27.7% of HS patients seemed to suffer from acne, respectively. In addition, there have been reports of HS associated with keratitis–ichthyosis–deafness syndrome. One patient exhibited congenital deafness, palmoplanta keratoderma, itchthyosiform scaling, follicular hyperkeratosis, and mild keratitis in addition to dissecting cellulitis of the scalp, cystic acne, and HS. In this patient, genetic analysis revealed a point mutation in a gap junction protein, connexin 26. This demonstrated a potential genetic link between these 2 syndromes, because mutations in connexin 26 have been involved in syndromes associated with both sensorineural deafness and hyperkeratotic skin disorders. It is likely that the abnormal keratinization associated with keratitis–ichthyosis–deafness syndrome leads to the follicular plugging seen in follicular occlusion disorders.
Dowling–Degos disease is an autosomal dominantly inherited genodermatosis that presents with spotted, reticular pigmentation on the flexural surfaces. Dowling–Degos disease is also related to follicular plugging and the coexistence of these conditions may be explained by the commonly shared pathogenesis of follicular occlusion as well as the distribution on the body. One case series in 1993 found that 8 of 21 patients (38.1%) with Dowling–Degos disease also had HS. Additionally, 6 other cases have described this association. Last, scarce literature has proposed a link between HS and Down syndrome.
Rheumatologic Comorbidities
An association between rheumatologic joint conditions, namely spondyloarthopathies and synovitis, arthritis, pustulosis, hyperostosis, osteitis (SAPHO) syndrome has been seen in conjunction with HS. Similar to the theory of pathogenesis related to antigenic exposure from compromised physical barriers, Jemec and colleagues proposed that the development of these rheumatologic comorbidities may be owing to cutaneous antigen exposure that is not usually encountered systemically. These antigens may induce inflammation and antibody complexes that get deposited in the synovial fluid, inciting inflammatory, sterile arthropathy.
Spondyloarthropathies were first described by Wright in 1978 as a group of seronegative (negative rheumatoid factor) arthropathies including psoriatic arthritis, ankylosing spondylitis, arthritis of IBD, and reactive arthritis. The commonalities between these spondyloarthropathies include being seronegative with sacroiliitis/spondylitis, peripheral mono/polyarthritis, genetic predisposition, and extraarticular manifestations of the skin, mucous membranes, eyes, and internal organs. Although the first association of HS and spondyloarthropathies was reported in 1978, it took approximately 30 years before a prospective evaluation of this association was published. This prospective evaluation was performed as a multicenter, observational study of 640 patients with HS. Consistent with much of the HS demographic data, the study population had a mean age of 39.4 years, 80% female, 70% current smokers, and the mean BMI was 29.4 kg/m 2 , and the distribution of Hurley stages were 16% I, 38% II, and 44% III. Of the 640 HS patients, 184 (28.8%) had musculoskeletal symptoms, 43 (6.9%) had evidence of arthritis, enthesitis, or inflammatory back pain, and 24 (3.7%) were diagnosed with spondyloarthropathy after evaluation by x-ray, MRI, and a rheumatologist. Of patients with both HS and joint pain, the HS preceded joint pain in 90% of cases by a mean of 3.6 years. Of arthritic patients also assessed for HLA-B27, 9 of 16 (56.3%) were HLA-B27 negative.
In a retrospective study of 29 cases of HS and spondyloarthropathy, involvement of axial (69%) and peripheral (86%) joints was common. The knee was the most frequently affected peripheral joint (59%). In a prospective study of 44 patients with HS and seronegative spondyloarthropathy, there were no differences in HLA antigen frequencies compared with a control group. A prior case series on these conditions reported axial joint involvement in 10 of 10 cases, peripheral joint involvement in 8 of 10 cases, and cutaneous manifestations preceding arthritic symptoms in 8 of 10 cases.
The diagnosis of SAPHO syndrome includes: (1) sterile acute or chronic joint inflammation with (a) pustolosis, (b) acne, or (c) hidrandenitis suppurativa; (2) multifocal, noninfectious osteomyelitis; (3) sterile monoosteitis or polyosteitis. In SAPHO, it is thought that chronic exposure to common cutaneous bacterial agents may promote desensitization, permitting low virulence infection or artherogenic stimulants resulting in arthritis and osteitis for genetically susceptible individuals.
In a prospective HS study from Richette and associates, 4 of 640 patients (0.63%) were identified as having SAPHO. The prevalence of SAPHO in the general population has never been characterized, but estimates are around 0.01% to 0.04%. In 2002, Steinhoff and colleagues reported a case series of 12 patients with SAPHO and 7 (58.3%) also had HS. Additional cases of these comorbid conditions have been reported in the literature.
Malignancies
Concern for HS-associated malignancies first arose from the discovery of squamous cell carcinomas (SCC) within or neighboring HS lesions in 3.1% to 3.2% of evaluated HS patients. A retrospective study of 2119 patients with HS found a 50% increased risk of cancer of all types compared with the standard incidence of cancer in the Swedish population being studied. Specifically, nonmelanoma skin cancer, buccal cancer, and primary liver cancer were significantly increased in these patients. However, the authors did note that buccal and liver cancers might be disproportionately increased owing to uncontrolled confounders. Given the significantly elevated risk of nonmelanoma skin cancer arising in HS lesions, examiners should raise their index of suspicion for malignancy and lower their biopsy threshold in HS patients to prevent or minimize SCC metastasis.
In 2011, Losanoff and colleagues reviewed 64 cases of SCC arising in HS and reported 2 new cases. They found that most SCCs were diagnosed 20 to 30 years after HS and the prevalence varied by anatomic distribution: 37% gluteal, 29% perianal, 21% perineal, 10% thigh, and 3% groin and trunk. No cases have been reported in the axilla.
Scheinfeld proposes that the development of malignancy occurs owing to a synergistic effect between the chronic inflammation of HS, impaired cellular immunity, and the presence of the human papillomavirus. Chronic inflammation is associated with malignant transformation in a number of other conditions (eg, Crohns disease, Marjolin’s ulcers), and thus could be a contributory factor to the development of SCCs in HS. Prolonged inflammation, decreased tumor suppressor activity, and decreased innate immunity in HS skin are likely causative factors. One case series of HS lesions had positive human papillomavirus test in all 8 cases evaluated; 7 of these 8 cases were positive for the high-risk subtype, human papillomavirus-16. After the use of biologics in the management of HS, additional concerns regarding precipitating the development of SCC have developed. However, it is unclear whether or not there is a causal relationship. A metaanalysis of 74 randomized controlled trials with anti–TNF-α biologics failed to confirm or refute that short-term anti–TNF-α agents caused an increase in the development of malignancy.
Other Somatic Complications
Additional complications to HS have been suggested, for example, anemia, amyloid, and most recently renal hyperfiltration.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


