Key points
• Select an access incision that will provide the most direct route to the underlying bone.
• A coronal incision can be used to access the cranial vault, forehead, zygoma, orbit, nasal dorsum, temporomandibular joint (TMJ), and condylar/subcondylar regions.
• The Gillies approach is an incision that allows a blunt instrument to be placed deep to the zygomatic arch.
• The upper blepharoplasty approach provides greater access to the superolateral rim compared with the lateral eyebrow approach. This may be a longer incision but is nicely concealed in patients with deep-set upper tarsal creases.
• To access the inferior orbital rim, floor of the orbit, and superior edge of the anterior maxilla, a subciliary or transconjunctival incision is used.
• A submandibular (Risdon) incision may be used to expose the inferior mandible.
• Retromandibular approaches expose the posterior ramus. The authors prefer a retroparotid approach.
Anatomy
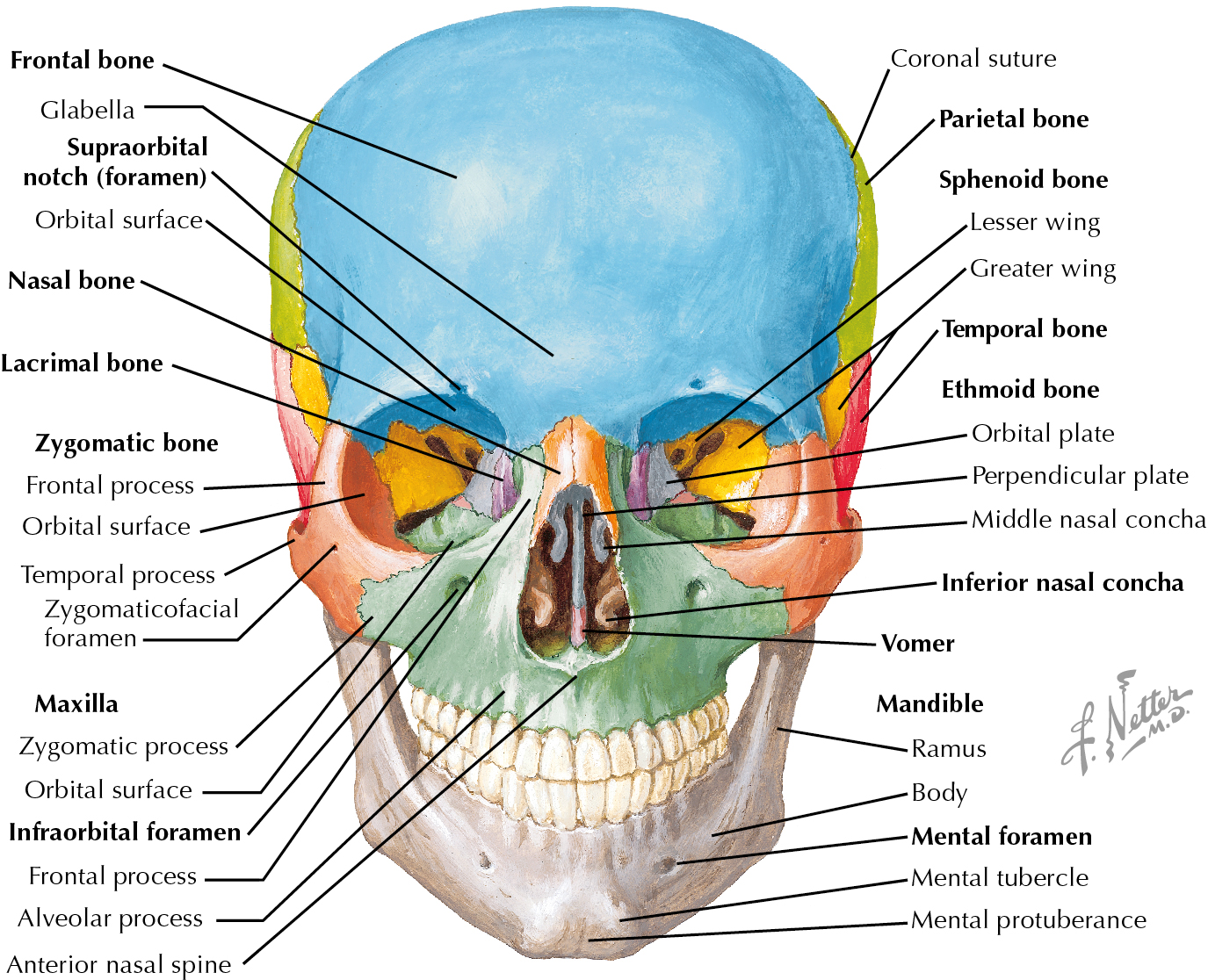
The face is composed of bony and soft tissue components, both of which are important to form and function. The soft tissue of the face will be primarily discussed in this chapter; however, understanding the skeletal anatomy is crucial. The skull or cranium is the skeleton of the head and is made up of two subdivisions: neurocranium and viscerocranium. The neurocranium provides the covering of the brain and comprises the calvaria and the cranial base. The calvaria are made up of the frontal, parietal, and occipital bones. The sphenoid and temporal bones help make up the cranial base. The ethmoid bone primarily is a part of the viscerocranium but makes a small contribution to the skull base. The viscerocranium or facial skeleton is composed of 15 bones that make up the mouth, jaws, nasal cavity, and eye sockets. Midline bones include the mandible, ethmoid, and vomer. Lateral to this are the maxilla, inferior nasal conchae, zygomatic bones, palatine bone, and lacrimal bone. The mandible and the maxilla house teeth and make up the oral cavity. The facial skeleton is commonly divided into the lower, middle, and upper thirds. The lower facial skeleton primarily consists of the mandible. The midface is composed primarily of the maxilla, and the upper third of the face primarily comprises the frontal bone ( Fig. 10.1 ).
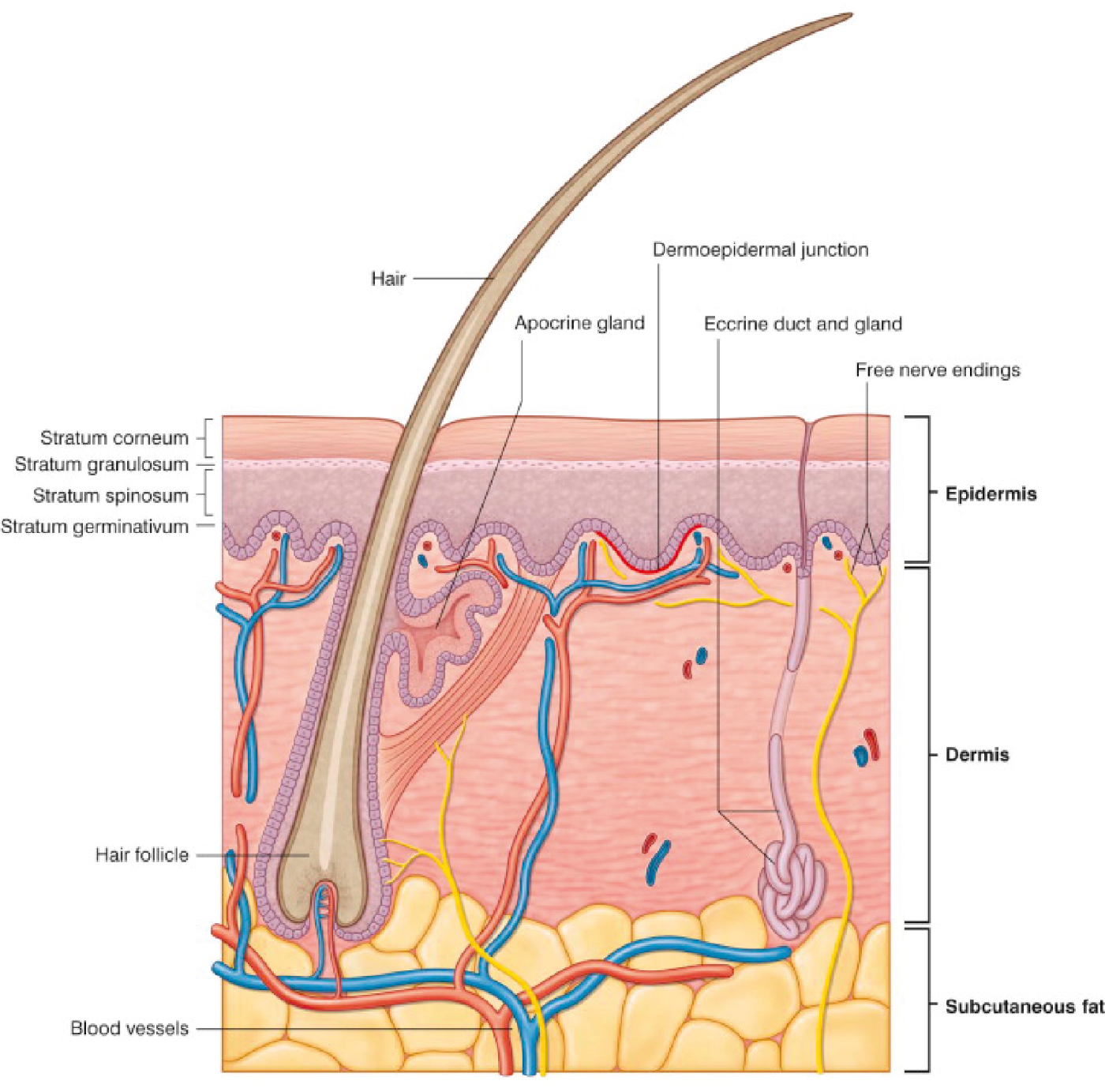
The soft tissues of the face have many components. Facial skin is made of the epidermis and the dermis ( Fig. 10.2 ). Facial skin varies widely from one person to the next and with age, but the thickness of the skin tends to be proportionate among people. The nasal tip skin tends to be 3.3 times thicker than the eyelid skin. The brow/forehead and nasal dorsum is 2.8 and 2.9 times thicker than the eyelid skin, respectively. The intrinsic elasticity of the skin is important for surgeons to understand. The dermis can be inflexible on the back and scalp, and small degrees of rotation can result in protrusion at the pivot point, whereas with areas with much elasticity, such as the face, tissue can be moved with greater ease and malleability. Intrinsic tissue elasticity is based on many factors: age, photodamage, and anatomic location. Below the skin is the subcutaneous fat, which is organized into compartments with the help of retaining ligaments. Subcutaneous fat, its compartments, and the retaining ligaments of the face are all crucial components to dissection and surgical manipulation. The subcutaneous fat of the face has been studied and found to be highly compartmentalized, and aging of the face is likely a combination of laxity of the retaining ligaments, volume loss, and malposition of the compartments of the face. Understanding the anatomy of the fat compartments and retaining ligaments is essential for surgeons.
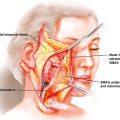
The fat compartments of the midface can be better appreciated by understanding their relationship to the zygomaticus major muscle ( Fig. 10.3 ). Its origin is at the anterior aspect of the zygoma, and it inserts on the modiolus near the corners of the mouth. The nasolabial fat compartment lies anterior to the medial cheek fat and overlaps the jowl fat. Its inferior border is the zygomaticus major muscle. Three major cheek fat compartments have been described: medial, middle, and lateral temporal cheek fat. Medial cheek fat has boundaries, which include the medial border nasolabial fold, orbicularis retaining ligament superiorly, jowl fat inferiorly, and lateral orbital compartment. The middle cheek fat pad is lateral to the medial fat pad and is anterior and superficial to the parotid gland. Middle cheek fat and medial cheek fat fuse to make a dense fascial network, called the zygomatic ligament , which abuts the parotideomasseteric ligament. The lateral temporal cheek compartment is the most lateral and is superficial to the parotid gland. It connects temporal fat to the cervical subcutaneous fat. The lateral cheek septum, a true septum, is anterior to this compartment and is encountered during a preauricular facelift.
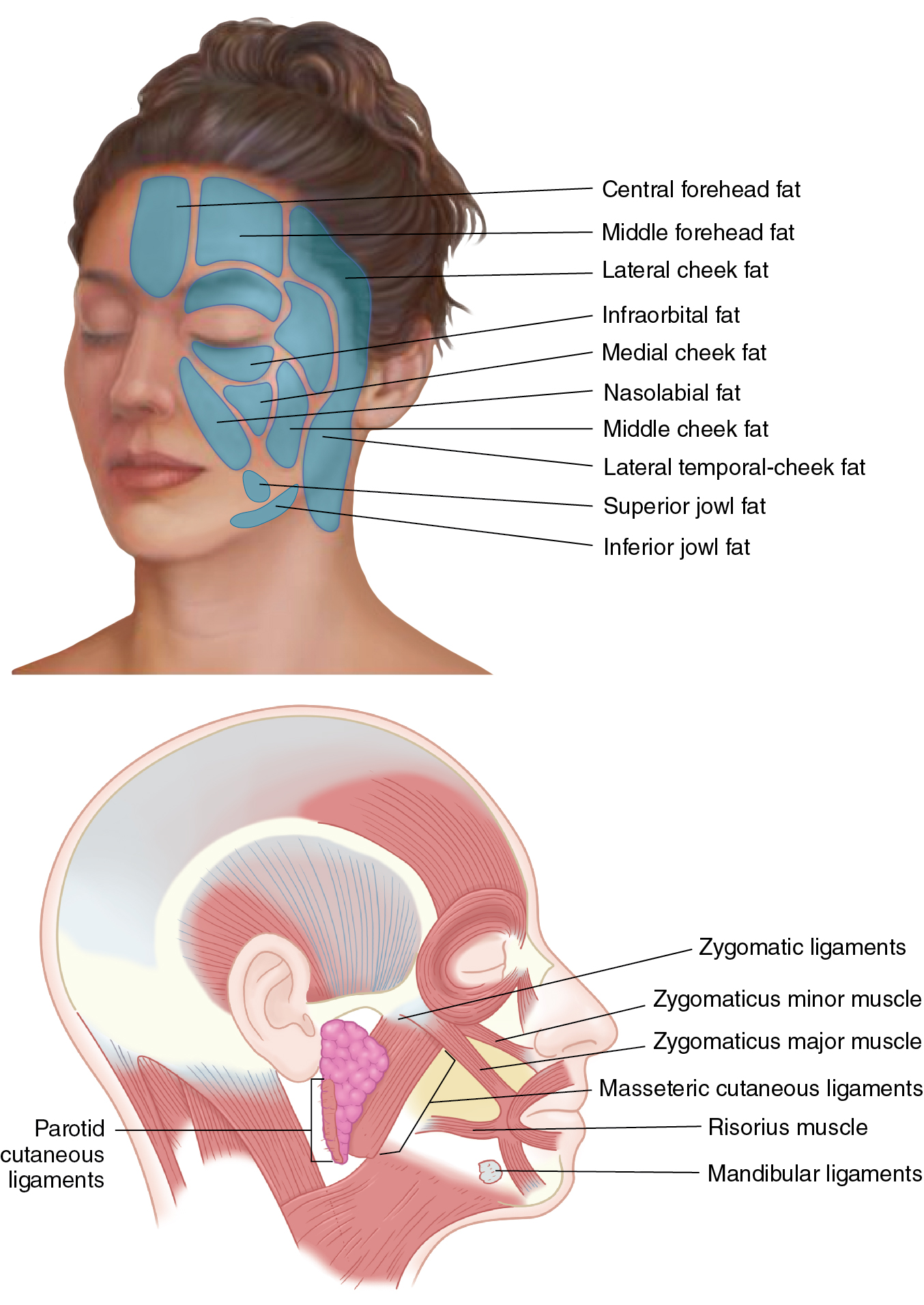
The forehead has three fat compartments. The central compartment is midline; it is inferiorly bounded by the nasal dorsum and laterally by the central temporal septum. The middle temporal fat compartments lie lateral to the central compartment, with the inferior border being the orbicularis retaining ligament, and are laterally bound by the superior temporal septum.
Orbital fat compartments are divided into three compartments around the eye. The superior compartment is superior in the globe and bounded by the medial canthus, lateral canthus, and orbicularis retaining ligament. Inferior orbital fat is inferior to the lid tarsus and bounded by the orbicularis retaining ligament (malar septum) and bilateral canthi. The lateral orbital fat compartment is bounded by the inferior temporal septum, zygomaticus major muscle, and orbicularis retaining ligament.
The jowl fat compartment adheres to the depressor anguli oris muscle and is medially bordered by the lip depressor muscle and inferiorly by membranous fusion of the platysma (mandibular ligament).
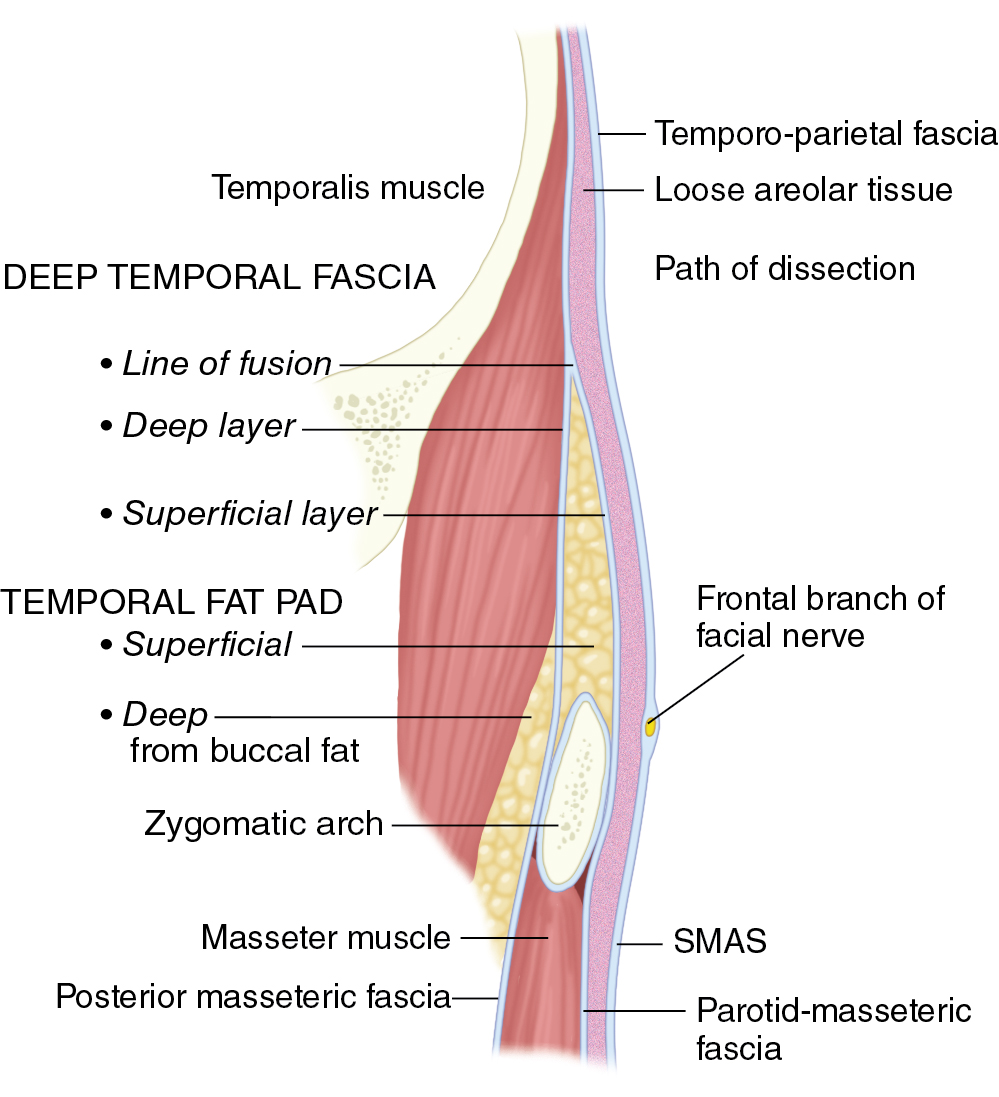
Knowledge of the nerves of the face is important in dissection, and these nerves should be avoided, when possible. Injury to the frontal branch of the facial nerve has a reported incidence as high as 20%. The frontal branch is thought of as a single nerve, but it has been shown that it comprises 2 to 5 rami, with connections to each other. These branches cross the central third to half of the zygomatic arch, and these interconnections likely lead to return of function when injury occurs. The trajectory of the frontal branch has been discussed by Pitanguy as coursing 0.5 cm below the tragus to 1.5 cm above the lateral brow. The sentinel vein can be used as a landmark with anatomic studies finding the frontal branch approximately 6.8 mm cephalad. The frontal branch above the zygomatic arch lies just deep to the temporoparietal fascia ( Fig. 10.4 ). Safe dissection is either superficial to the temporoparietal fascia or deep to or on the superficial leaf of the deep temporal fascia.
The buccal branch is the most commonly injured facial nerve branch, although there is significant arborization. Injuries are usually compensated for by the multiple rami or the connections with the zygomatic or marginal mandibular branches. The buccal branches are prone to injury due to their proximity to the retaining ligaments, with the most commonly injured buccal branch just inferior and lateral to the zygoma. For safe dissection in this region, the surgeon should dissect both above the upper zygomatic ligaments and 5 mm below the upper masseteric ligaments to stay in the plane superficial to the superficial musculoaponeurotic system (SMAS). The marginal mandibular branch carries a high risk of injury due to lack of much redundancy in rami. The path of the nerve usually exits the anterior caudal margin of the parotid and stays deep to the parotid–masseteric fascia and deep cervical investing fascia. As it crosses the mandible, it stays deep to the platysma and deep fascia. It crosses superiorly over the posterior digastric muscle, submandibular gland, and facial artery. The lower masseteric ligament is a region where this nerve can be injured because these attachments make it easy to enter the wrong plane deep to the platysma and injure this nerve. By staying superficial to the SMAS and platysma, the surgeon can avoid injury to this nerve. The cervical branch is commonly injured and mistaken for a marginal mandibular injury. Most commonly, it is injured when the nerve becomes superficial near the midline, and it can be distinguished from a marginal branch injury by the patients’ ability to pucker the lips. There is arborization of the nerves; therefore almost all patients regain their function.
The trigeminal nerve supplies the majority of sensation to the face. The supratrochlear and supraorbital nerves are terminal branches of the ophthalmic division (V1) of the trigeminal nerve and supply sensation to the upper eyelid and forehead. The supraorbital nerve exits though the supraorbital notch or foramen of the superior orbital rim. The supratrochlear nerve exits medial to the supraorbital nerve on top of the supraorbital rim. The maxillary division (V2) gives off the infraorbital nerve, which exits the infraorbital foramen and supplies sensation to the majority of the midface. The mental foramen of the mandible is where the mental nerve (distal branch of the inferior alveolar nerve, V3) exits. Its location is typically described as inferior to the second premolar.
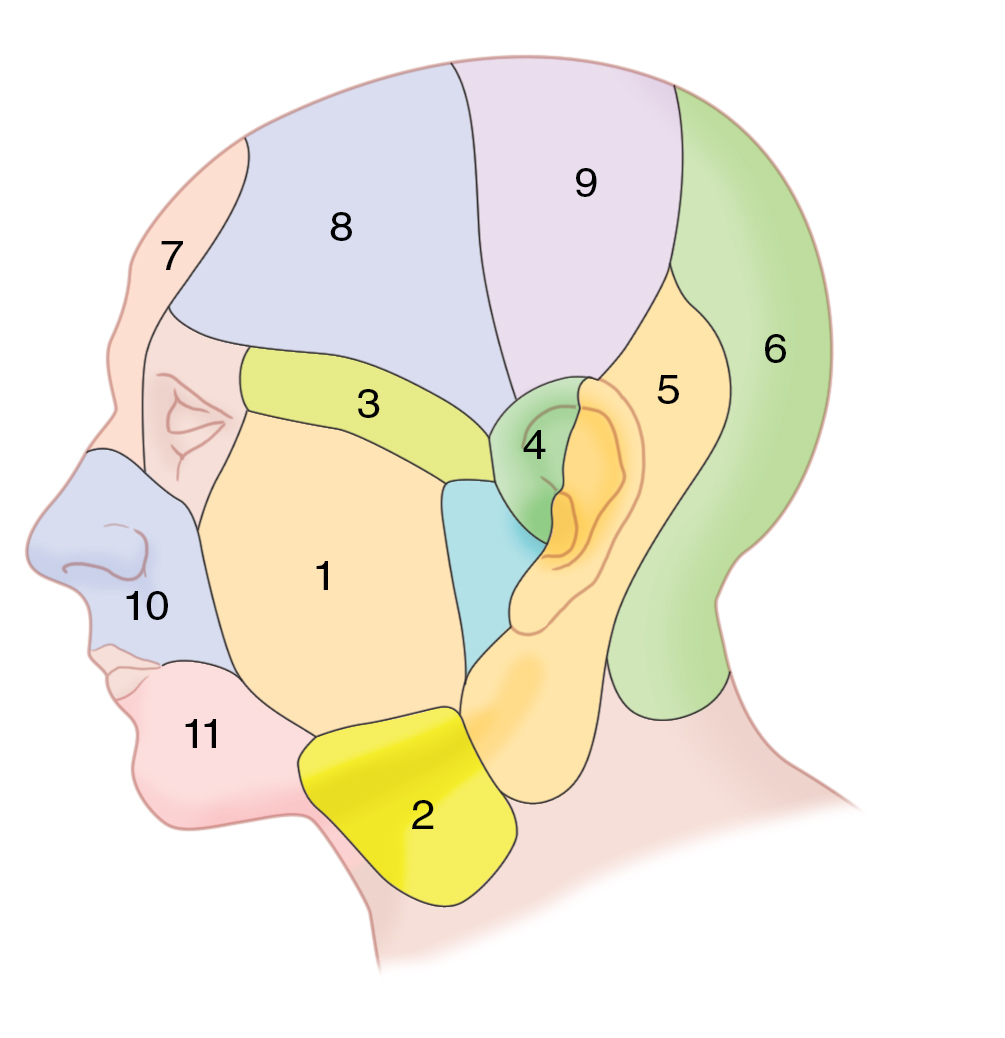
Mathes et al. evaluated the arterial anatomy of the face and territories of cutaneous perforating vessels. They found that there are 11 defined vascular territories to the face and scalp ( Fig. 10.5 ). These territories are supplied primarily from separate arteries: transverse facial, submental, zygomatico-orbital, anterior auricular, occipital, supratrochlear, superficial and parietal branches of the superficial temporal, and superior and inferior labial arteries. These territories have three patterns of arterial vascularization: (1) small densely populated musculocutaneous perforating arteries supplying the anterior face, (2) large sparsely populated fasciocutaneous perforators that occur in predictable locations supplying the lateral region of the face, and (3) small densely populated fasciocutaneous perforators supplying the scalp. The deep circulation of the anterior face (facial artery and supratrochlear artery) courses deep to or through the facial muscles. Those vessels perforate the subdermal plexus through small, fine musculocutaneous arteries. The lateral face deep circulation (transverse facial, submental, and posterior auricular arteries) is in the parotideomasseteric plane and perforates the subcutaneous plane in constant sites and then undergoes further branching once in the subdermal plexus. The scalp vessels run superficial to the galea, and a dense population of vessels perforates the superficial fascia of the scalp and supplies the dermis and skin.