Subplatysmal Neck Lifting
Dino Elyassnia
Timothy Marten
DEFINITION
A well-contoured neck is an artistic imperative to an attractive appearance.
A good neckline conveys a sense of youth, health, and vitality and lends an appearance of sensuality and beauty (FIG 1).
Neck improvement is of high importance to almost every patient seeking facial rejuvenation, and the results of our face-lift procedures are largely judged by the outcome of the neck.
Traditional neck lift techniques do not adequately address many aspects of aging in the submental region, and it is not enough in most situations to limit treatment to preplatysmal lipectomy alone or with postauricular skin excision. Subplatysmal problems will contribute significantly to aging and require treatment in most cases if optimal results are to be obtained (FIG 2).
ANATOMY
It is critical to understand the distribution of fat in the cervicosubmental region. Cervical fat is present in three distinct layers—preplatysmal, subplatysmal, and deep interdigastric fat.
Subplatysmal fat will be evident as a centrally situated triangular shaped fat pad with its base lying at the hyoid and tip near the mentum (see TECH FIG 1A). The two sides of the triangle will lie along each digastric muscle. Deeper interdigastric fat is situated in between and deep to the plane tangent to the anterior bellies of the digastric muscles.
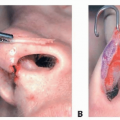
The submandibular gland (SMG) is a lobulated, pink to tan-colored structure covered by a smooth capsule. It sits in confined space with the anterior belly of the digastric muscle lying medial, the mandibular border lateral, and the mylohyoid muscle deep (see TECH FIG 2A). The superficial and deep lobes are separated by the mylohyoid muscle.
Important neurovascular structures will all lie extracapsular to the gland, so intracapsular dissection is safe. The marginal mandibular nerve will lie superior and lateral to the SMG. The facial artery and vein will lie in close proximity with the vein passing superficial and the artery deep to the gland. An intraglandular perforator artery arising from a branch of the facial artery will be found within the posterior portion of the superficial lobe in a central location.
 FIG 1 • Patient seen before and after neck lift. A good neckline conveys a sense of youth, health, fitness, sensuality, and beauty. The patient has also undergone a face-lift, foreheadplasty, eyelid surgery, and fat injections. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Success or failure in treating the neck lies in the ability of the surgeon to identify the anatomic basis of patient problems and to form a sound surgical plan for their correction.
A focused history should include all previous cosmetic treatments for the neck including previous neck lift or noninvasive treatments like Thermage, Ulthera, Kybella, etc.
Obtain any history of dry mouth or Sjogren syndrome as this is a relative contraindication to reduction of the prominent SMG.
The cervicosubmental region of each patient must be carefully examined both at rest and during platysmal activation to distinguish between soft adynamic cervical bands and dynamic hard bands. This is best accomplished by asking the patient to “push the jaw forward and tighten the neck.” Soft bands change little during activation and are predominantly a problem of loose skin or platysmal laxity, whereas hard bands become tight or exaggerated and indicate a problem of platysma hyperfunction (FIG 3).
Evaluating the location of fat in the neck is also made easier by palpating the neck with and without platysmal activation. Fat lying predominantly in a preplatysmal position will generally feel “soft” and remain in the examiner’s grasp upon platysmal activation. However, fat in a subplatysmal location will have a firmer feel and will tend to be pulled superiorly out of the examiner’s grasp when the platysma is contracted (FIG 4).
SMGs are usually palpable as firm, smooth, discrete, mobile masses in the lateral submental triangle. Large glands
requiring treatment are most readily visible in the secondary face-lift patient who has had prior aggressive lipectomy; however, they can be more hidden in the primary patient with a full neck and must be palpated to ascertain their size and need for treatment (FIG 5).
A small subgroup of patients will present with large, bulky anterior bellies of their digastric muscles that are evident on visual exam as linear paramedian submental fullness. These are most often seen in the secondary face-lift patient who has had prior aggressive lipectomy (FIG 6). However, in the typical primary patient, it is difficult to assess their size; thus, the decision to treat these muscles is usually made intraoperatively.
 FIG 2 • Patient seen before and after neck lift. A careful evaluation of the preoperative photo shows platysmal laxity, excess subplatysmal fat, large submandibular glands, and digastric muscle hypertrophy. Removing subcutaneous fat and tightening skin over these anatomic problems do not correct them and cannot produce the type of improvement shown here. |
IMAGING
Typically, radiographs are not necessary in facial rejuvenation surgery.
All patients should have standardized photographs taken preoperatively, and any markings made preoperatively on patients should be photographed as well.
These photos should be used intraoperatively to help guide treatment.
NONOPERATIVE MANAGEMENT
Some limited options exist to treat isolated problems in the neck.
Neuromodulators can be used to treat dynamic platysmal bands. Some have reported success using neuromodulators to partially reduce the size of SMGs, but results have been mixed at best.
Deoxycholic acid (Kybella) is an injectable medication recently approved for reduction of submental fat. Also, CoolSculpting has been approved for the same treatment. At this point, it is unclear if these treatments are only affecting the subcutaneous fat or also having an impact on subplatysmal fat. Significant reduction of subcutaneous fat is likely not appropriate for most patients in the typical face and neck lift age group. Thus, like submental liposuction, use of these newer treatments should probably be limited to younger patients with discrete subcutaneous fat excess in the submental area.
 FIG 3 • Dynamic assessment of the cervicosubmental region. The neck is examined in repose (A) and as the platysma is contracted (B). Dynamic platysma muscle irregularities are often referred to as “platysma bands.” |
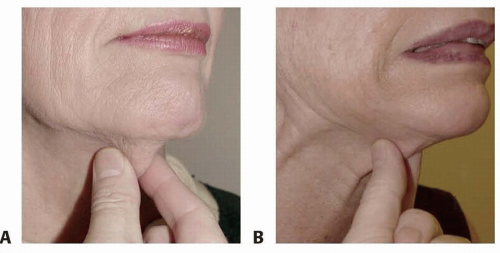 FIG 4 • Assessing the location of cervicosubmental fat. A. Submental “waddle” is grasped with the face and neck in repose. B. The patient is then asked to activate the platysma muscle. In this example, fat is pulled superiorly from the examiner’s grasp indicating a predominantly sub platysmal position. Fat lying predominantly in a subcutaneous, preplatysmal position would tend to remain within the examiner’s grasp when the platysma is activated. |
SURGICAL MANAGEMENT
Traditional neck lift techniques that focus on preplatysmal lipectomy, skin excision, and platysmaplasty do not adequately address many aspects of aging in the submental region. For many patients, subplatysmal fat accumulation, SMG enlargement, and digastric muscle hypertrophy will contribute significantly to the neck deformity and necessitate additional treatment.1,2
In all but the unusual or young patient, the majority of cervical fat accumulates in a subplatysmal location, and little if any will need to be removed from the preplatysmal layer. As patients age, fat stores generally shift from a preplatysmal location to a subplatysmal one. The small amount of subcutaneous fat present must be preserved to maintain a soft appearance to the neck.
Large SMGs often contribute to the appearance of a full, “obtuse,” and “lumpy” neck. Glands protruding inferiorly to a plane tangent to the ipsilateral digastric and the mandibular border are likely to be problematic if excess cervical
fat is removed, platysma is tightened, and excess skin is removed. These glands warrant reduction, and the protruding portion can be incrementally resected through the submental incision.
The decision to perform SMG reduction should be made in conjunction with the patient after appropriate discussion of the benefits versus risks. Patients should know that the procedure may prolong submental induration and carries a small but unlikely risk of bleeding, sialoma, salivary fistula, and dry mouth. Patients should also be informed, however, that only the protruding portion is excised and the majority of the gland is left in place.
Once treatment of subplatysmal fat and SMGs has been performed, the anterior bellies of the digastric muscles should be evaluated. If the muscle bellies are deemed to be prominent intraoperatively, subtotal digastric myectomy should be performed. Failure to evaluate bulging of these muscles after other modifications of the submental region can lead to an unexpected and objectionable submental bulge postoperatively.
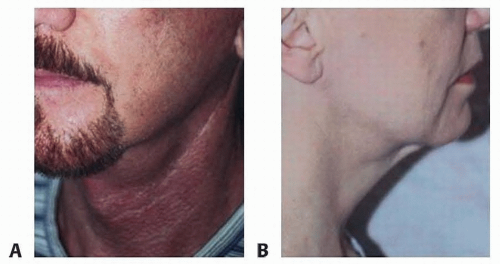 FIG 5 • Prominent submandibular glands. Submandibular glands are usually evident as protruding masses in the lateral submental triangle, lateral to the anterior belly of the ipsilateral digastric muscle. A. Patient with residual prominent submandibular gland after face-lift and submental liposuction. His prior procedure has made the prominent glands more obvious. B. Patient with residual prominent submandibular gland after “weekend neck lift.” Aggressive resection of subcutaneous fat has exposed the prominent gland. |
 FIG 6 • Prominent anterior belly of the digastric muscle. The patient has had prior face and neck lift. The anterior belly of the digastric muscle can be seen as objectionable linear paramedian fullness in the submental region that spoils an otherwise good result. Prominent digastric muscles often go unnoticed at the time of the primary procedure due to the fact that they are frequently hidden by cervical fat and lax platysma muscle. (Courtesy of T. J. Marten, MD, FACS.) |
Preoperative Planning
All patients undergo a preoperative physical evaluation, and patients with significant medical problems must be cleared by their internist.
Patients are required to avoid all medications or supplements that increase the risk of bleeding for 2 weeks prior to surgery.
The majority of our neck lifts are performed under deep sedation administered by an anesthesiologist using a laryngeal mask airway (LMA). This allows the patient to be heavily sedated but still maintains spontaneous breathing without compromise of the airway.
The flexible LMA is also particularly useful in neck surgery. When this device along with the breathing circuit is draped separately, it can be moved side to side during surgery giving unobstructed access to the submental region.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree