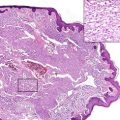
Fig. 64.1
SPTCL: Infiltrated deep-seated skin lesions on the neck with ulceration (Courtesy of Prof. Dr. G. Burg, Zürich)
Pathology
SPTCL is characterized by lobular infiltrates composed of small- to medium-sized lymphoid cells with nuclear pleomorphism (Figs. 64.2 and 64.3). The rimming of adipocytes by tumor cells is a consistent feature, but is not disease-specific. Karyorrhexis and cytophagocytosis may be present. The tumor cells express CD3+ CD4- CD8+ CD56- phenotype and cytotoxic proteins such as TIA-1+, granzyme B+ and perforin (Fig. 64.4a) and show a high proliferative activity (Fig. 64.4b). By definition, expression of TCR alpha/beta has to be demonstrated by immunohistochemistry (betaF1). There is no association with Epstein-Barr virus (EBV). Clonal rearrangement of the alpha/beta chain of the T-cell receptor is found.
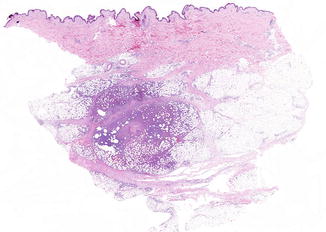
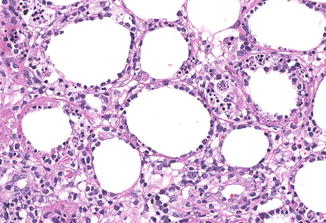
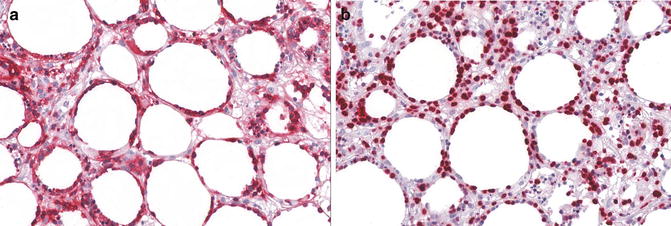
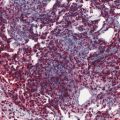
Fig. 64.2
SPTCL: Lobular infiltrates in the subcutis (Note absence of infiltrates in the dermis)
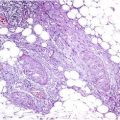
Fig. 64.3
SPTCL: The adipocytes are surrounded by neoplastic lymphocytes with moderately chromatin dense nuclei (so-called rimming)
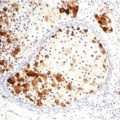
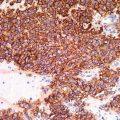
Fig. 64.4
SPTCL: Expression of CD8 (a) and high proliferative activity (Ki67) (b) by the tumor cells
Differential Diagnosis
SPTCL has to be distinguished from subcutaneous form of GD-TCL, which shows overlapping histological features with predominantly lobular infiltrates of atypical lymphocytes of varying size. In contrast to SPTCL, GD-TCL exhibits expression of TCR gamma/delta (TCR gamma+ or TCR delta+) and in most cases CD56. Extranodal T/NK-cell lymphoma, nasal type, can be differentiated by the expression of CD56 and EBV. Lupus panniculitis lacks significant atypia of lymphocytes and shows often lymphoid follicles with reactive germinal centers and clusters of CD123+ plasmacytoid dendritic cells. In individual cases, however, differentiation between lupus panniculitis and SPTCL may be very challenging, especially since occurrence of both disorders has been observed in the same individuals. Rarely, subcutaneous infiltrates in the context of Borrelia infection can mimic SPTCL. The relationship of SPTCL to cytophagic histiocytic panniculitis (CHP) remains to be clarified, especially since some cases of CHP may represent SPTCL.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


