- •
Subcutaneous adipose tissue, once considered a passive storage receptacle with a fixed number of cells and limited purpose, is now recognized as a complicated organ with important endocrine and metabolic functions
- •
Both increased and decreased adipose tissue mass as seen in obesity, anorexia and lipodystrophy, have profound effects on multiple body systems such as the immune, reproductive and hematopoietic systems
- •
Mature adipocytes exist as two main types: white and brown adipocytes that are distinguished by differences in their color and function and have distinct vascular and nerve supplies
- •
Treatment options for subcutaneous fat (excess or atrophy) can be broadly categorized as either nonsurgical or surgical
Introduction
Although it is well accepted by dermatologists that subcutaneous fat is an essential component of the skin, the basic science of fat physiology is still a poorly understood ‘black hole’ in the field of dermatology. Medical disorders related to fat such as panniculitis, lipodystrophies, localized adiposity, and atrophy are commonly treated by dermatologists either by medications or surgical procedures. The demand for procedures that manipulate fat especially for cosmetic enhancement is becoming increasingly popular.
Multiple conditions affect fat distribution in the human body. Studies have shown the association between severe obesity and mortality due to increased rates of cardiovascular disease and diabetes. The type of regional adipose tissue with excess body fat in the upper mid-section of the body called android or male-type obesity represents the entity called visceral obesity. The type of fat distribution associated with accumulation in the lower part of the body or gluteofemoral region is known as gynoid or female type obesity, the excess of which is associated with higher grades of cellulite.
General adiposity (assessed by body mass index [BMI] which is determined by weight/height ) and abdominal adiposity are associated with a higher risk of death. However, abdominal obesity, which is determined by waist/hip ratio, may be a stronger indicator of obesity than BMI. Visceral and subcutaneous fat have distinct features and excess of either of these may result in a variety of health-related and/or aesthetic concerns.
Subcutaneous fat and gluteofemoral (cellulite) fat
The topographic anatomy of fatty tissue includes two layers that are separated by a superficial fascia. The more external layer or areolar layer consists of vertically oriented globular large adipocytes. The deeper layer, known as the lamellar layer, has horizontally arranged smaller cells with larger and more numerous blood vessels. Women and children tend to have a thicker areolar layer, which, in turn, is thicker in the gluteofemoral regions. Fatty tissue development during puberty is more robust in women than in men. This may be explained by the influence of estrogen as 17β-estradiol stimulates the replication of adipocytes ( Fig. 5.1 ). The adipocytes in the gluteofemoral region are larger and are influenced by female sex hormones These adipocytes are also metabolically more stable and resistant to lipolysis. In addition, estrogen increases the response of the adipocytes to antilipolytic α 2 -adrenergic receptors (α 2 -ARs).
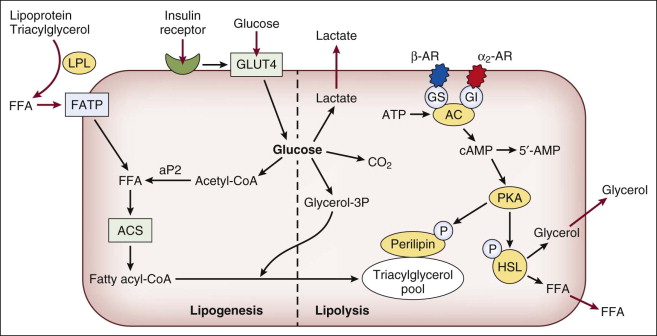
The only hormones that are able to affect lipolysis in human adipocytes are catecholamines (epinephrine and norepinephrine, which are lipolytic) and insulin (antilipolytic). Functionally, there are marked regional differences in both hormonal responsiveness and metabolic activity of human adipose tissue. Catecholamine-induced lipolytic responsiveness is greater in viscera than in abdominal subcutaneous tissue and gluteofemoral fat cells. The regulation of lipolysis by catecholamines involves AR stimulation of adenylate cyclase via β-ARs (β 1 , β 2 , and β 3 -ARs) and inhibition by α 2 -ARs ( Fig 5.1 ). Abdominal and gluteal adipocyte cell size correlates directly with α 2 -AR density (p < 0.1). The fact that the ratio of α 2 -AR to β-AR is higher in the gluteal region than in abdominal adipocytes accounts for some of the enhanced responsiveness of abdominal fat cells compared with gluteal fat cells to mixed AR agonists, such as epinephrine and norepinephrine. In addition, abdominal adipocytes have a greater sensitivity to pure β-AR agonists such as isoproterenol. These factors are responsible for enhanced lipolysis of abdominal adipocytes secondary to catecholamine stimulation as compared to gluteal adipose tissue.
Catecholamine-induced lipolytic responsiveness is greater in visceral fat than in the gluteofemoral or so-called cellulite-prone areas.
Adipose tissue lipoprotein lipase (LPL) directly correlates with the adipose cell size and its affinity for β-AR. Catecholamine-induced lipolysis, as measured by localized LPL release, suggests that abdominal adipocytes have an abundance of β-AR with greater central obesity seen in post-menopausal women as opposed to gynoid feminine type obesity, which is more prevalent in pre-menopausal women. Exogenous estrogen has been shown to have an inconsistent effect on lipolysis. For instance, it was shown to decrease LPL activity in the lower body of pre-menopausal women and yet have the opposite effect in postmenopausal women, again accounting for greater rates of central obesity seen after menopause. Gluteal fat cells are larger in size and richer in α 2 -AR in pre-menopausal and post-menopausal women undergoing hormone replacement therapy.
White and brown adipocytes
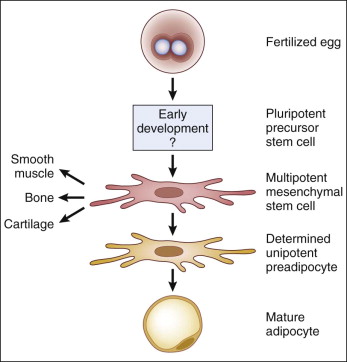
Adipocytes are organized in a ‘multidepot organ’ with only one-third of adipose tissue containing mature adipocytes. The remaining two-thirds consist of a combination of nerves, fibroblasts, and adipocyte precursor cells, or pre-adipocytes ( Fig. 5.2 ). Mature adipocytes exist as two cell types, white adipose tissue (WAT) and brown adipose tissue (BAT), that are distinguished by their color and function. WAT is yellow or ivory and contains predominantly white adipocytes. BAT, which appears brown, contains multilocular brown adipocytes. Compared with WAT, BAT contains a richer vascular tree and denser capillaries in combination with mitochondria, which accounts for its ‘brown’ color. Both types of adipose tissue are innervated by the noradrenergic sympathetic nervous system.
Mature adipocytes can be distinguished as either white adipose tissue (WAT) or brown adipose tissue (BAT) with distinct histologic and functional characteristics. Histologically WAT is made up of spherical cells of a wide size range (15–150 µm diameter). The size range is wide due to variation in amount of lipids stored in the lipid vacuole of the adipocyte. Additional cells present within both BAT and WAT include vascular endothelium and neural cells comprising neurovascular bundles supplying it as well as fibroblasts, histiocytes, and mast cells. BAT is made up of smaller 10–25 µm round cells with a cytoplasm rich in mitochondria. Unlike WAT, lipids are stored in small vacuoles within BAT adipocytes and glycogen is abundant. All of these features correspond to the functional differences between the two adipose tissue types. BAT and WAT represent different adipose cell types and have somewhat opposing functions in the body. While WAT acts as an energy storage depot, the main function of BAT is thermogenesis, which involves energy expenditure. Despite these differences in function, it is not unusual to find small islands of BAT within WAT. Furthermore, in states of obesity, BAT can lose its thermogenic function and take on morphological features of WAT.
BAT and WAT are histologically distinct yet interchangeable. Lipids in WAT are organized within one large, ‘unilocular’ droplet, the size of which exceeds 50 µm. White adipocytes are spherical, allowing for maximum volume expansion within minimal space. The nucleus is compressed to one side because of the high lipid content. Lipids within brown adipocytes are organized into multiple smaller, multilocular droplets. They have higher mitochondrial content packed with cristae within the cytoplasm. Cells are polygonal, have centrally placed nuclei, and are relatively smaller than WAT, ranging from 20 µm to 40 µm.
WAT is distributed in several anatomically distinct and separate collections or ‘depots’, namely the subcutaneous and intra-abdominal, each with its own characteristic metabolic, endocrine, paracrine, and autocrine function ( Table 5.1 ). In humans, BAT is most abundant in newborns and neonates. However in adults, it is also found around many major vessels, in perinephric fat pads and near adrenal glands. In small mammals, such as rodents, BAT persists throughout life. In larger mammals and humans, BAT depots undergo a morphologic transformation in which they rapidly accumulate fat, become unilocular, and lose the ultrastructural and molecular properties that define them, including mitochondria. Because of this, there are very few, if any, collections of BAT in adult humans.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


