Static facial sling procedures are one of many facial reanimation options to address long-standing and irreversible facial paralysis. The primary goals of static reanimation are to provide symmetry at rest and improve static function at repose. Choosing the best option depends on patient factors, such as age, comorbidities, and injury factors. Different materials are available for static sling surgery; we believe autologous tendon offers the most reliable and long-lasting results. Static suspension procedures provide immediate results, improved resting position, and can augment other techniques. This article discusses available options for static reanimations to address the eye complex, midface, and mouth.
Key points
- •
The main goal of static reanimation is to restore symmetry at rest.
- •
Palmaris or plantaris tendon graft static suspension provides long lasting results compared to other static suspension materials.
- •
Treatment of levator palpebrae superioris hyperactivity should be done through tightening and elevating the lower eyelid rather than placing a heavier upper eyelid weight.
- •
Brow lift and eyelid weight procedures should not be done at the same time.
- •
Addressing both upper and lower eyelid laxity is important to treat excessive tearing.
Introduction
Facial paralysis has devastating consequences emotionally, aesthetically, and functionally. , Facial reanimation treatments are broadly divided into reinnervation, static, and dynamic. Static procedures can provide symmetry at rest and the illusion of facial tone but do not offer movement. These procedures do not provide symmetry during function.
Facial paralysis management needs to be considered based on location and degree of functional loss. It may involve the entire face or different anatomic units, such as the brow, upper eyelid, lower eyelid, midface, and lower lip. Paralysis is either complete or partial loss of function and it is reversible or irreversible based on the cause of nerve/muscle injury. Paralysis is generally considered irreversible if present for longer than 2 years or when the distal nerve/motor unit is not present.
Among the goals of restoration for the irreversibly paralyzed face is to achieve symmetry and improve static function, such as oral competence in repose. This involves static suspension of the oral commissure and lateral ala to recreate a nasolabial fold. In this article we focus on the static approaches for facial reanimation.
Many static procedures have been described to treat the paralyzed face. Choosing the best option depends on patient factors, such as age and comorbidities, and injury factors, such as duration, location, and prognosis. The approaches for static suspension also depend on whether the procedures will be performed at the time of ablative surgery or as a secondary procedure.
Table 1 summarizes the static reanimation procedures discussed in this article.
| Region | Technique |
|---|---|
| Brow | Direct brow lift |
| Upper eyelid | Eyelid weight Lateral tarsorrhaphy |
| Lower eyelid | Lateral strip canthopexy Lower eyelid suspension with tendon |
| Nasal base | Alar base suspension |
| Midface | Nasolabial fold suspension |
| Mouth | Oral commissure suspension |
| Upper/lower lip | Tendon suspension |
Material
A variety of materials have been used during static procedures including suspension sutures; alloplastic materials (eg, Gore-Tex); acellular dermal matrix; and native tissues, such as fascia or tendon grafts. ,
The palmaris or plantaris tendons have become our preferred material because of their tendency to resist laxity and maintain their position over time. These tendons are easily harvested at the time of ablative surgery and have the benefits of being native tissue. The palmaris tendon is easily identified on clinical examination. In patients who are missing this tendon, other options include plantaris or the long extensors of the toes (third or fourth). Note that the plantaris longus tendon may also be absent in some patients.
For midface resuspension, a longer tendon is often required. As a result, the plantaris longus is the preferred option. Preoperative MRI or intraoperative exploration is performed to identify the tendon.
Advantages of using tendon grafts include: resistance to lengthening, lower relapse rate, very long sling (eg, plantaris longus), and minimal to no donor deficit. However, a separate donor site scar is required.
Eye complex static procedures
The immediate priority in managing a patient with facial paralysis is ensuring adequate corneal protection. This is important regardless of whether or not the paralysis is reversible. The eye complex is considered in three segments that include the brow, upper lid, and lower lid.
Brow ptosis can cause a reduction in the visual field and asymmetry and upper eyelid paralysis can lead to corneal dryness and exposure. This in turn can cause epiphora and pain and may lead to corneal ulceration.
Lower eyelid paralysis results in poor tear film maintenance and drainage leading to epiphora. With time, this lower eyelid laxity results in scleral show and ultimately to ectropion further worsening corneal exposure, epiphora, and pain.
Excessive tearing is a common symptom that is bothersome for patients with facial paralysis. The causes of excessive tearing include: (1) corneal exposure, dryness, and irritation because of poor upper lid closure; (2) loss of lower lid support with the puncta falling away from the globe resulting in inefficiency in the canalicular system; and (3) loss of the pump action of the orbicularis oculi on the lacrimal sac affecting normal drainage. , ,
Improvement in upper eyelid closure may reduce symptoms of irritation and thereby excessive lacrimation. However, better upper lid function alone does not address the tear drainage system. Therefore, addressing the position and tone of the lower eyelid should be considered to reduce epiphora.
We consistently see an improvement in upper lid closure following lower lid tendon suspension. The exact mechanism of this finding is unclear but may be related to a transmission of tension laterally from the lower lid to the upper lid. As a result, we often stage the two procedures. Lower lid suspension and tightening is generally performed first followed by upper lid weight insertion. This approach has allowed us to downsize the weight needed for appropriate upper lid closure.
Direct Brow Lift
A brow lift may be indicated for aesthetic or functional deficits. Eyebrow ptosis may result in facial asymmetry or visual field impairment secondary to excess upper eyelid skin.
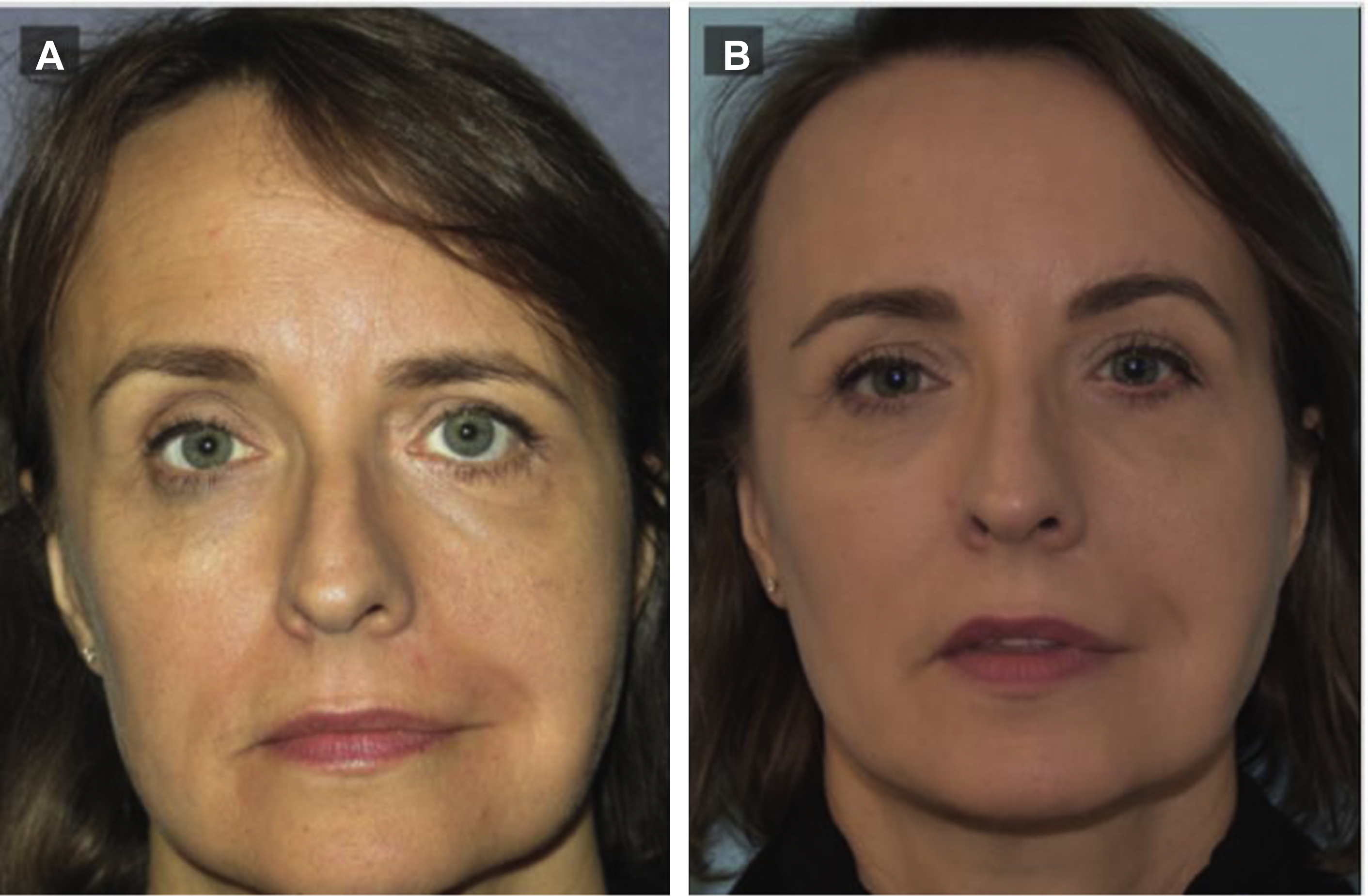
Direct brow lift, unlike other techniques, such as midforehead lift, coronal incision, and endoscopic brow lift, is simple, quick, and repeatable with immediate results. It can also be performed under local anesthetic. Especially in patients with irreversible paralysis, a direct brow excision provides the best long-term outcome with a lower rate of relapse. This procedure can also be combined with botulinum toxin injections on the contralateral side for added symmetry even during motion. The one disadvantage to this approach is an external scar just above the brow, which is more visible in younger patients or those with less brow hair Fig. 1 .
This procedure should be performed with caution when performed simultaneously with an upper eyelid procedure, such as weight insertion or blepharoplasty, because brow elevation can reduce eyelid closure.
Upper Eyelid Weight
Upper lid weight insertion is indicated in patients with symptomatic incomplete upper eyelid closure and provides a significant reduction in lagophthalmos and improvement in corneal coverage. Upper lid loading with either a gold or platinum weight as a static procedure is simple, safe, effective, and reversible. Compared with gold, platinum weights have a thinner profile and cause less foreign body reaction, which can improve esthetics and lower the risk of extrusion; however, they are more expensive.
Some patients over time can develop hyperactivity of the levator palpebrae superioris muscle. These patients often present with progressively poorer upper lid closure despite weight insertion. We have found that lid closure is most effectively improved in these patients by lower lid tightening and suspension rather than replacing an existing weight with a heavier one.
Lateral Tarsorrhaphy
Lateral tarsorrhaphy is a simple and reversible procedure that is done under local anesthetic. Indications include: a temporary measure to protect the cornea while awaiting a definitive procedure to improve eyelid function, an emergency measure when there is the possibility of imminent visual loss caused by exposure, in combination with other eyelid procedures, or as a salvage procedure when other treatments have failed. Early intervention should be considered especially in patients with a poor or absent Bell phenomenon.
Lower eyelid
Lateral Strip Canthopexy
Lateral strip canthopexy is another static reanimation option for patients with mild to moderate lower lid laxity. These patients often present with scleral show or mild ectropion. This procedure only tightens the lateral two-thirds of the lid (lateral to the medial limbus) and therefore does not address any medial laxity. It is performed in isolation or in combination with a lower lid sling procedure if lid shortening is also necessary.
Lower Eyelid Suspension: Tendon Sling
Lower eyelid suspension with tendon sling is our preferred procedure for patients with moderate to severe ectropion. Unlike a lateral strip canthopexy, the tendon sling addresses medial and lateral lower lid laxity and can also tighten and further suspend the medial canthal tendon. Young patients with mild lid laxity, patients with relative proptosis (positive vector), or malar hypoplasia are relative contraindications for this procedure. Specifically, patients with a negative vector can have the lid/sling migrate inferiorly under the globe worsening lid position so great care should be taken in this patient population.
Approach
A modified blepharoplasty incision (15–20 mm) within the medial aspect of the supratarsal fold is performed through the orbicularis muscle. Medial traction allows access to the periosteum of the nasofrontal junction and medial orbital wall, which is then incised and lifted. This allows exposure of the medial orbital wall, nasofrontal junction, and supraorbital rim.
A lateral canthotomy incision is performed to access the lateral orbital wall. The periosteum of the lateral orbital rim is incised and elevated allowing exposure of the lateral orbital rim and internal lateral orbit. In cases when the lower lid is also lax, a lateral tarsal strip procedure can also be performed, which allows shortening of the lid by 5 to 8 mm.
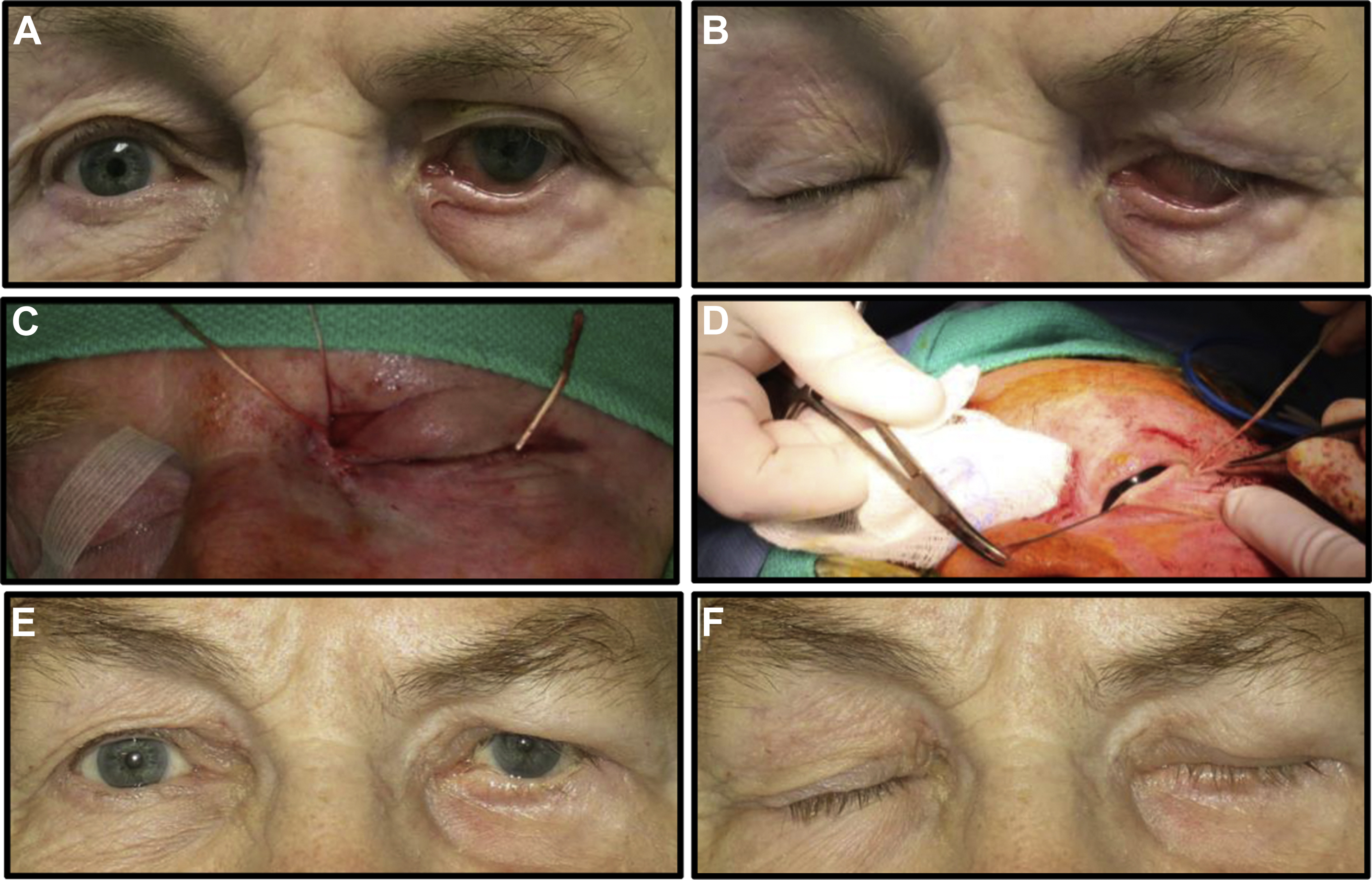
Once harvested, the tendon is split using a scalpel into a 1- to 2-mm-thick strip. The harvested mini tendon is threaded along the ciliary margin of the lower lid using a Keith needle. The needle is prebent to better follow the gentle curve of the eyelid. The needle is brought out of the skin just lateral to the inferior punctum. The needle is reinserted through the same puncture site, allowing a change in direction. It is passed either through the medial canthal tendon, or deep to it avoiding the canalicular system ( Figs. 2 and 3 ).
Related posts:
 Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
 Modified Selective Neurectomy
Modified Selective Neurectomy
 Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
 Dual Nerve Transfer for Facial Reanimation
Dual Nerve Transfer for Facial Reanimation
 Reinnervation with Selective Nerve Grafting from Multiple Donor Nerves
Reinnervation with Selective Nerve Grafting from Multiple Donor Nerves
 Treating Nasal Valve Collapse in Facial Paralysis
Treating Nasal Valve Collapse in Facial Paralysis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


