Chapter 69 Stability Results After Anterior Cruciate Ligament Reconstruction
The primary purpose of anterior cruciate ligament reconstruction (ACLR) is to restore knee stability. This chapter will provide meta-analytic data on hamstring, bone–patellar tendon–bone (BPTB), quadriceps tendon, and allograft stability. The stability data are measured by instrumented Lachman testing, usually but not exclusively KT-1000 (Medmetric, San Diego, CA). Pivot-shift data are not included because the high interobserver variability makes it impossible to quantify and it is an insensitive test in the nonanesthesitized patient.1 Although it is theoretically possible to have normal stability with instrumented Lachman testing and still have a pivot slide or even pivot shift present, this can only happen if the graft is put in a very vertical position. The data in this chapter are from the peer-reviewed literature, and the authors of these studies are all accomplished knee surgeons who are unlikely to place vertical grafts. Thus the data shown should be a good index to the relative stabilities of the knees tested.
Statistical Methods
Meta-analytic methods were used to compare the groups. Weighted means for normal and abnormal stability were generated as follows: For each treatment group, the proportion of individuals for an outcome event was determined by adding the number of events that occurred through all studies and dividing by the number of the patients in all the studies. The number of patients for any single-center, but not multi-center, study was capped at 100 to avoid disproportionate influence of any given study. In any study, if the number of patients for a given outcome was not recorded, the study was eliminated from the analysis of that outcome. For example, with one exception, if a study did not record the number of patients who have less than 2 mm of difference, then the study was not included in the <2 mm comparison.2–66
Results
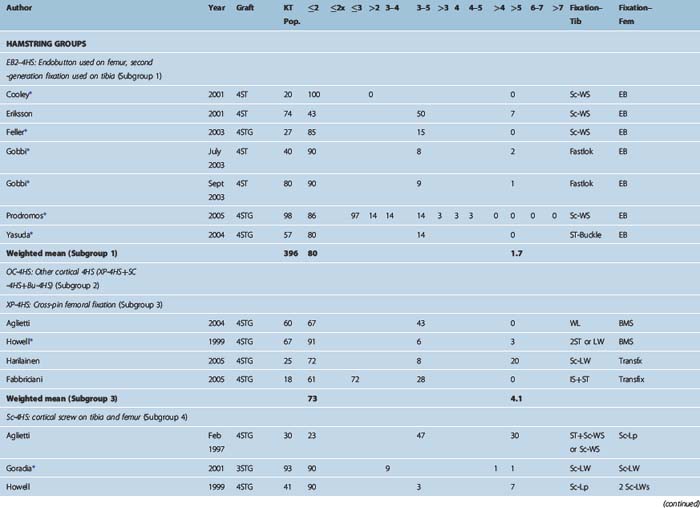
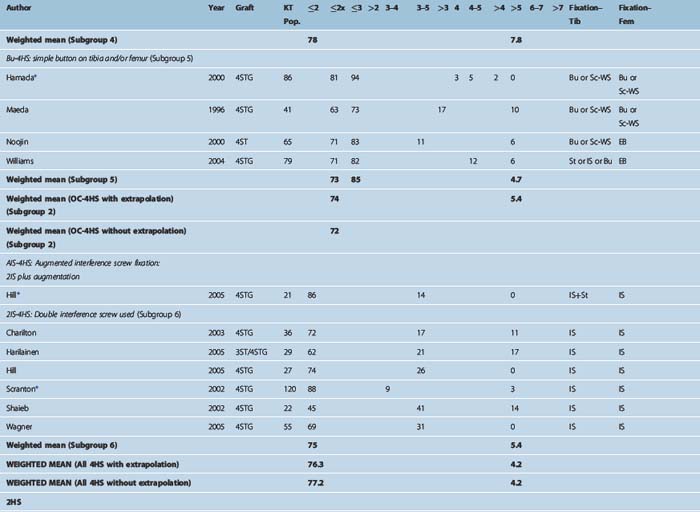
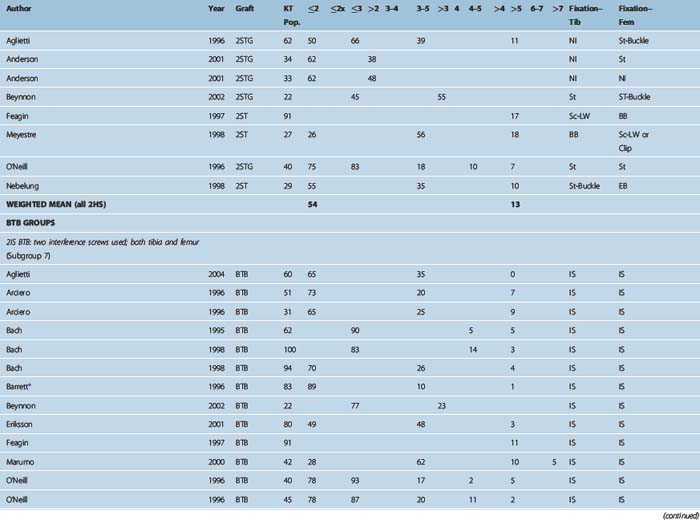
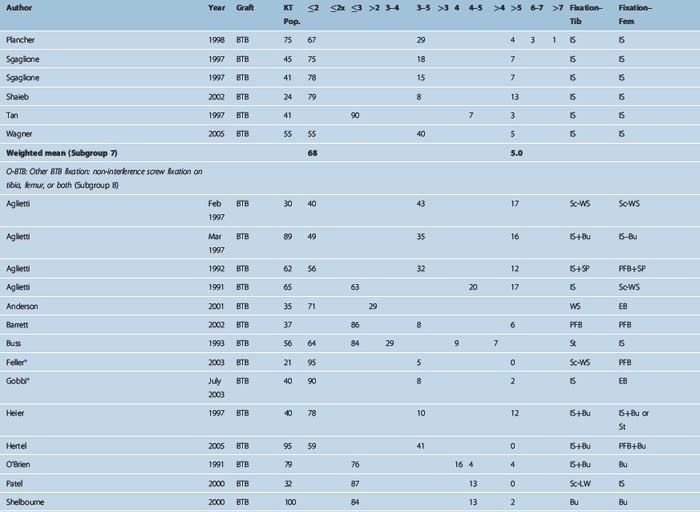
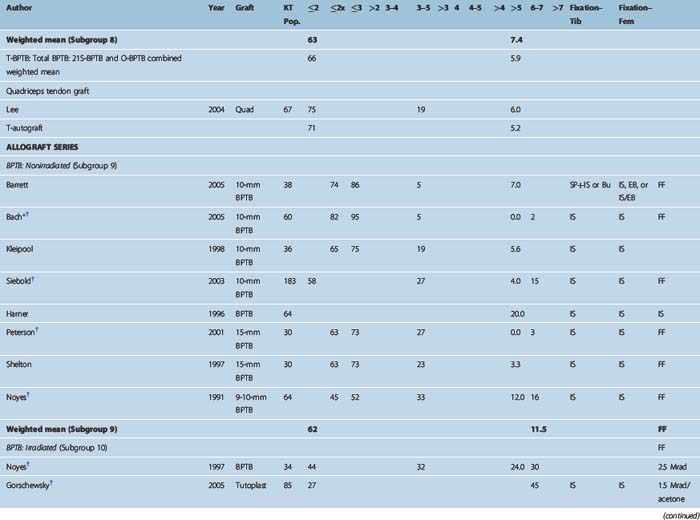
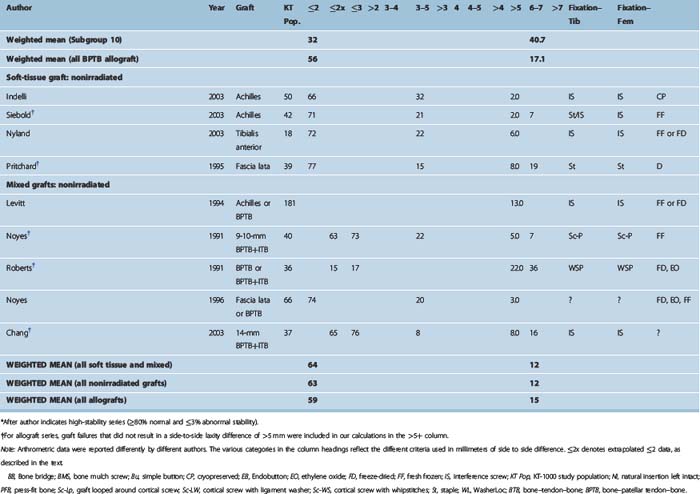
Table 69-1 shows all studies broken down by graft and then by fixation type for all graft types.
Only About Half of Reconstructed Knees Achieve Stability Symmetrical with the Other Knee
The goal of ACL surgery is to restore the preinjury level of stability, which should be the same as that of the other knee. True symmetry is achieved when the side-to-side difference (SSD) between the knees is 0. Measurement error increases this criterion to 1 mm. Thus we propose a SSD of 1 mm as defining knee stability symmetry. The IKDC “normal” criterion of up to a 2-mm difference may be satisfactory, but it is not truly normal. Indeed, a 2-mm SSD is what is commonly seen with partially torn ACLs.67 When the 1-mm criterion is applied, we see the following: For all autografts, about 30% have greater than 2-mm SSD.68 The remaining 70% fall into four categories: 2 mm, 1 mm, 0, or less than 0. If we assume that one-fourth of the 70% falls into each of these four categories, then it is reasonable to estimate that one-fourth of 70%, or 18%, are exactly 2 mm different. Adding this 18% (exactly 2 mm) to the 30% (greater than 2 mm) would mean that 48% of the reconstructed population has a 2-mm or greater SSD. This leaves about 52% with 1 mm or less SSD (i.e., true symmetry with the other knee). Thus roughly one-half of the autograft ACLRs, in the hands of the experienced knee surgeons who are the authors of these studies, have stability that is either equivalent to a partially torn ACL or worse. The allograft data68 show significantly lower stability rates (see Table 69-1).
Table 69-1 presents the raw data for stability from all the studies. The principal areas of interest are the “normal” and “abnormal” stability columns. Abnormal stability in most cases is equivalent to graft failure. The primary table subdivision is by graft type. These are four-strand hamstring (4HS) autograft, two-strand hamstring (2HS) autograft, BPTB autograft, and quadriceps tendon autograft and allograft. The secondary subdivision is by graft subgroup and by fixation type. Subdividing by fixation groups is possible to do with the autografts because of the large number of studies. It is only possible with the allografts to break out a BPTB/interference subgroup because of the smaller number of studies.
Stability Rates by Graft Type
The principal findings were as follows:
Stability Rate by Graft Fixation Subgroups
Stability rates for these subgroups are as follows:
Aperture Versus Nonaperture Fixation
For soft tissue grafts, there was no stability advantage for aperture fixation. Indeed, as just described, the 4HS-EB2 group, which had entirely nonaperture cortical fixation, had the highest stability rates of any graft fixation subgroup. Thus the so-called “bungee effect” would appear to be nonexistent. This is not surprising, as studies have shown that fixation on rigid cortical bone enhances stiffness much more than the greater length of the construct diminishes it.69 Also, variations in fixation stiffness are eliminated once the graft heals into the bone tunnel because the fixation is no longer load bearing. What really matters is how much the graft may elongate during this healing period from either slippage or plastic deformation. Neither of these is related to fixation stiffness.
Four-Strand Hamstring Versus Bone–Patellar Tendon–Bone Stability Rates
Because BPTB has long been considered the “gold standard” for ACLR. it may be surprising to some that 4HS was found to have higher stability rates. However, as the 4HS graft is a significantly stronger graft (see Chapter 10), the excellent 4HS stability rates do make sense if modern fixation is used. Prior analyses have seemed to show that hamstring grafts had lower stability rates than BPTB.70,71 However, these studies commingled the much-lower-stability 2HS studies with the higher-stability 4HS studies. If the 2HS studies are removed, it turns out that there was no stability advantage to BPTB in those studies by comparison with 4HS. Also, many of the highest-stability 4HS series were published after those studies. They were thus not included in those analyses but contribute significantly to the higher 4HS stability rates found here.
Allograft Versus Autograft
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


