Fig. 29.1
(Above) Preoperative patient with idiopathic facial atrophy. (Below) One-year postoperative large-volume traditional syringe-harvested fat grafting (100 mL) performed in 1988
Fournier referred to this technique as “Microlipoextraction et microlipoinjection” [7]. Today, many different techniques have evolved for transferring liquified fat, but there is no standard procedure that is widely accepted. Harvesting, washing, spinning, digesting, mixing, and PRP have all played an important role in the quest for better survival of our transplanted fat. In recent years, Lee [8] has made important contributions in the area of autologous fat grafting. Because of Lee’s advances, the author has developed a new paradigm for facial rejuvenation, and this is the basis for this chapter.
29.2 Early Introduction to Adivive™ (Lipokit™)
Lee developed the Lipokit™ system through his company Medikan International. Lipokit appealed to the author because it was simple, totally enclosed, and with relatively inexpensive disposables. The Lipokit Fat Processing Unit (FPU) proprietary name from Medikan was changed to Adivive™ in December 2011, but the unit is still produced by Medikan. Since the production of the 18.75-cm-diameter centrifuge system, Medikan now produces specialized harvesting syringes for smaller volumes.
29.3 Equipment and Technique Used with the Adivive™ FPU (Figs. 29.2, 29.3, 29.4, 29.5, 29.6, 29.7, 29.8, 29.9, 29.10, and 29.11)

Fig. 29.2
Adivive™ (Adivive™) Fat Processing Unit

Fig. 29.3
Adivive™ harvesting syringe with weighted piston
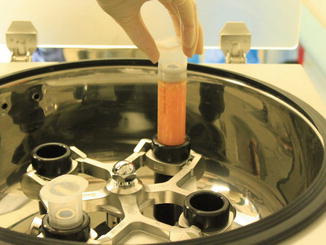
Fig. 29.4
Insertion of fat-filled syringe into sterile centrifuge bucket

Fig. 29.5
Centrifuged/filtered fat displaying three components

Fig. 29.6
Transferring processed fat into smaller syringes

Fig. 29.7
Droplet of processed fat

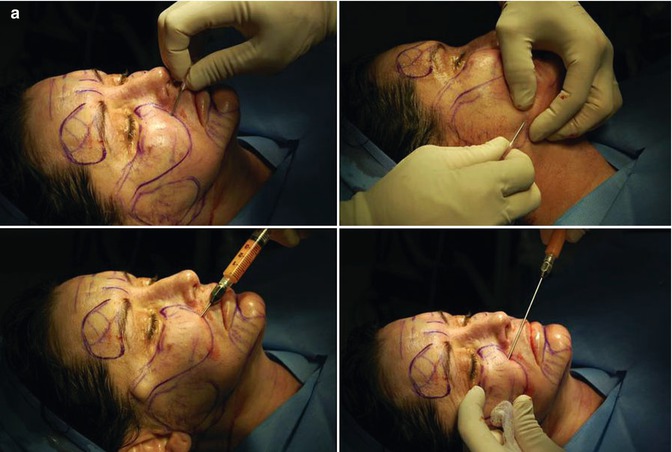
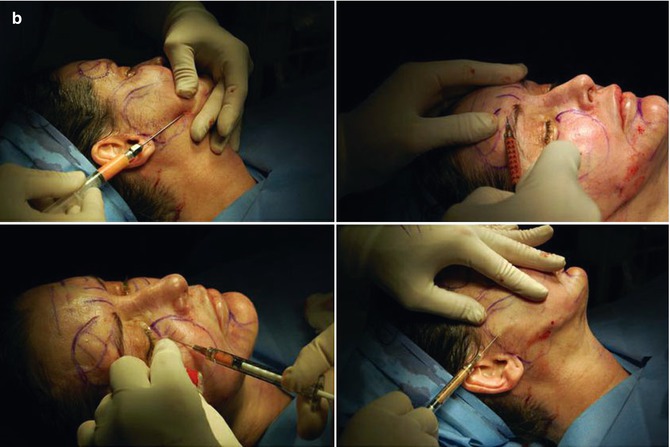
Fig. 29.8
Injecting patient with Adivive™ fat

Fig. 29.9
Magellan™ PRP processing unit

Fig. 29.10
Drawing blood for PRP processing

Fig. 29.11
Operating room, setup, and personnel
The Lipokit™ (Adivive™) Fat Processing Unit was developed by Medikan in 2004. Palomar acquired FDA clearance and imported the system into the United States at the end of 2010. In contrast to other systems, it is a totally enclosed unit from the point of infusion to harvesting, processing, and final delivery of the processed fat into the patient. Therefore, sterility and low risk of infection is one of the primary attributes of such a system. The wide-base centrifuge (18.75 cm) provides increased G forces during centrifuging inside a sterile bucket. The system includes a 60 mL sterile syringe with a weighted piston containing a unique filter. After spinning, the “lipocondensed” or “squeezed” fat remains in the center and the filtrate with tumescence and blood cells separates to the bottom. The oil squeezed from the fat ends up above the weighted piston and may be easily poured off. The plug at the bottom of the syringe contains a large number of stem cells and comprises the stromal vascular fraction (SVF). The average product of concentrated fat per syringe is approximately 30 mL which contains about one million stem cells per mL. The SVF plug is added to this purified fat. The author recently added PRP (platelet-rich plasma utilizing the Arteriocyte™ Magellan system) to the Adivive-purified fat graft for several reasons. The advantage of PRP is that it contains eight separate growth factors, millions of platelets, and an antibacterial component. It is thought that PRP enhances the take of the adipose-derived stem cell (ASC) graft. In addition, the millions of platelets present in PRP minimize bruising and edema, and the plasma facilitates injecting the thickened Adivive fat through small blunt cannulas. The PRP actually lubricates the condensed fat, and therefore, it is easier to inject in smaller strands.
The efficiency of the Adivive™ FPU is enhanced by integrating a well-trained team of technicians and assistants. The infusion and harvesting is performed and then the harvested fat is passed to the assistants. While the assistants process the fat, the author anesthetizes the face and neck. As soon as the fat is processed, the face is injected with the purified fat/PRP mixture. Simultaneous with infusion and harvesting, the nurse draws 60 mL of blood and spins it down to 6–9 mL of PRP. The fat is processed and mixed with PRP while the face and neck are anesthetized. Timing is critical so that the Adivive fat/PRP is grafted soon after it is prepared.
Additional treatments such as SlimLipo of the neck, brow lift, and facelifts are performed after the fat grafting is performed. With this type of team approach, 40–80 mL of graft material may be harvested, prepared, and delivered within a period of 60–90 min. With the addition of surgical procedures such as short incision facelift and brow lift, the total treatment time rarely exceeds 21/2 h.
29.4 Specifics Regarding Anatomic Placement, Graft Volume, and Cannula Size
Prior to surgery, careful markings are made with the patient in the upright position. The projected volume for each area is based on degree of soft tissue deficiency (Fig. 29.12), patient’s goals, and ancillary surgical procedures. The patient markings outline the areas of deficiency (Fig. 29.13). The neck markings were made in anticipation of neck tightening with the SlimLipo laser platform. The carotids and cervical branches of the facial nerve are marked as areas of avoidance, whereas the oblique lines are areas for intended skin tightening. The laser neck treatment avoids the need for submental platysmaplasty and effects a progressive post-laser neck tightening for at least 4–6 months.


Fig. 29.12
The anatomic basis of midfacial aging
Fig. 29.13
Preoperative patient markings
Cannula sizes, fat deposition depths, volume of fat injected, and 16-gauge needle access punctures are noted. The location and amounts of Adivive fat injected vary from patient to patient. An effort to establish fat volume needs as well as invasiveness of the procedure evolved into the Opera Lift nomenclature. The three categories established are designed to fit the cosmetic and economic goals of the patient. The various types of Opera Lifts will be defined later in this chapter.
More limited Adivive grafting sessions may require under 40 mL of processed fat. These limited procedures may be performed in an office setting using the smaller Adivive system. Larger volumes, especially if the fat grafting is performed in conjunction with surgical procedures, should be conducted in an operating room setting. With low-risk patients, most of these procedures are performed with monitored intravenous conscious sedation.
During the evolution of the Adivive FPU, the author found it useful to categorize patients based on the degree of complexity of the treatment plan. For many reasons, patients are requesting less invasive, less expensive cosmetic procedures with less downtime. Beyond the use of synthetic fillers and Botox™, Adivive and various lasers have added a whole new dimension to the practice. The categories used are largely based on the economic and treatment goals of the patient. The acronym “Opera Lift” may not be appropriate for other plastic surgeons, but this labeling has been useful in the author’s practice:
Opera (Obi-Palomar External Rejuvenation Aesthetic Lift) Minor, Opera Lift Major, and Opera Lift Plus are the categories the author has utilized during the past 18 months. Opera Lift is a proprietary name and not authorized by Palomar Medical. It stands for s.
29.5 Opera Lift Minor
The minor suffix indicates an office procedure using the minor Adivive system with one syringe of approximately 35 mL of processed fat. The patient is given Valium and Percoset preoperatively if requested, and the total procedure is performed in approximately 1 h. The donor site is first anesthetized (Fig. 29.14) followed by dental blocks (Fig. 29.15). Syringe harvesting is performed (Fig. 29.16) at one donor site and centrifuged at 2,500 rpm for 5 m. (Speed and duration of centrifugation is determined by BMI and the color of the aspirate.) For these cases, the Medikan™ short blunt 16–18-gauge disposable needles are extremely useful.

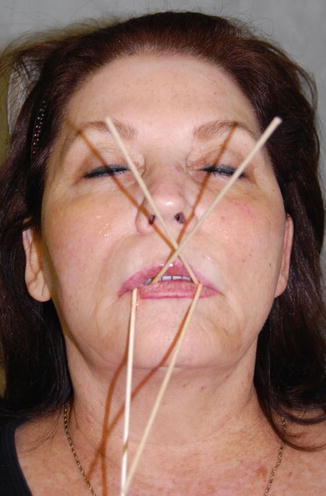

Fig. 29.14
Limited donor site with adequate fat
Fig. 29.15
Preparation for dental blocks
Fig. 29.16
Medikan™ small-volume harvesting device
With these limited volume procedures (30–35 mL), there is enough graft material to treat the glabellar lines, full tear troughs, malar regions, nasolabial folds, marionette creases, and lips (Fig. 29.17). Also, there is a better take with the smaller-volume procedures. Preoperative and postoperative oral Arnica Montana, avoidance of blood thinning substances, control of blood pressure, etc., is a universal treatment plan for all patients. Irrigation of the graft sites with ice saline delivered with the blunt needles (cannulas) at the end of the procedure significantly reduces bruising also. Levels of fat injections will be described under Opera Lift Major.
 Stem Cell Applications: An Overview
Stem Cell Applications: An Overview
 The Adipose Organ: Morphological Perspectives of Adipose Tissues
The Adipose Organ: Morphological Perspectives of Adipose Tissues
 The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
 Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
 Hand Rejuvenation with Stem Cell Fat Transfer
Hand Rejuvenation with Stem Cell Fat Transfer
 Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell




Related posts:
Stem Cell Applications: An Overview
The Adipose Organ: Morphological Perspectives of Adipose Tissues
The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
Hand Rejuvenation with Stem Cell Fat Transfer
Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
