Skin and composite grafting provide effective resurfacing and reconstruction for cutaneous defects after excision of the malignancy. The goal is to restore a natural appearance and function while preventing distortion of the eyelid, nose, or lips. With careful planning and attention to aesthetic subunits, the surgeon can camouflage incisions and avoid blunting aesthetically sensitive sulci. The surgical plan is also informed by the pathology, as basal or squamous cell carcinomas removed by Mohs micrographic excision have different prognostic and logistical considerations from melanoma. Skin and composite grafting are useful as stand-alone procedures or may complement local flaps and other soft tissue reconstructions.
Key points
- •
In Mohs reconstruction, full-thickness skin grafts are generally preferred over split-thickness grafts due to decreased contracture and improved color, contour, and texture.
- •
A variety of modifications to grafting technique can improve graft survival, restoration of normal contours, functional outcomes, and overall aesthetic results.
- •
Because grafts do not carry their own blood supply, optimizing recipient site conditions with a vascular bed is of paramount importance, particularly when performing composite grafts.
- •
Skin and composite grafts may be combined with other approaches to minimize distortion and optimize cosmetic subunits.
Overview of skin anatomy in relation to grafting
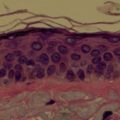
The skin is the body’s largest organ, and it varies widely in thickness and character across the anatomic regions of the face. Successful grafting is predicated on a basic understanding of this functional anatomy. The skin’s epidermis includes basal cell, prickle cell, granular cell, and keratin layers, and the epidermis attaches to the dermis via the basement membrane, which is the anatomic landmark that differentiates in situ or preinvasive lesions from invasive cutaneous malignancy. The dermis, in turn, affords skin most of it tensile strength. The dermis is penetrated by epidermal appendages, blood vessels, nerves, and cells. The richly vascularized and innervated pilosebaceous units include sebaceous glands, hair follicles, and arrector pili muscles that contain stem cells and have substantial regenerative potential. The fibroblasts found in the dermis facilitate wound contraction during healing and produce collagen, elastin, and ground substance. Epithelialization of cutaneous defects occurs from wound edges and the basement membrane along hair follicles and adnexal structures. Blood supply derives from both a deep subdermal plexus and a superficial plexus that supplies the superficial dermal papillae.
The skin serves a role as both graft and recipient in most cases of reconstruction. There are a variety of situations where skin grafts are indicated, and grafts are particularly useful for resurfacing superficial defects. Full-thickness skin grafts are also helpful in young patients who have tight skin and sizable defects that are not readily amenable to adjacent tissue transfer. Although skin grafts often minimize the need for additional facial skin incisions, they are susceptible to developing a “patchlike” appearance due to mismatch of color, contour, or texture if not carefully planned. Because of such concerns, skin grafts are used judiciously, proving especially useful in cases that cannot be reconstructed with a local flap or where major distortion would ensue. With thoughtful application of the principles presented herein, many patients can benefit from these aesthetic approaches. As evidence-based approaches evolve in facial plastics, grafting practices should become more consistent so as to achieve optimal outcomes.
Skin grafts may be harvested as full-thickness, split-thickness, or composite grafts with or without hair-bearing skin. The viability of the graft depends on the vascular supply to the recipient bed, thickness of the graft, appropriate compression of graft to recipient site, and patient factors, such as smoking, hypoxemia, diabetes, radiation, and history of prior surgery at the site. Exposed bone, tendon, and cartilage all decrease the probability of successful graft survival. Some irregularity at the junction of skin grafts and surrounding skin is common. When patients are routinely counseled preoperatively regarding the potential role for postoperative dermabrasion or other similar refinements, there is greater acceptance of procedures to achieve optimal match and camouflage of the reconstruction.
Overview of skin anatomy in relation to grafting
The skin is the body’s largest organ, and it varies widely in thickness and character across the anatomic regions of the face. Successful grafting is predicated on a basic understanding of this functional anatomy. The skin’s epidermis includes basal cell, prickle cell, granular cell, and keratin layers, and the epidermis attaches to the dermis via the basement membrane, which is the anatomic landmark that differentiates in situ or preinvasive lesions from invasive cutaneous malignancy. The dermis, in turn, affords skin most of it tensile strength. The dermis is penetrated by epidermal appendages, blood vessels, nerves, and cells. The richly vascularized and innervated pilosebaceous units include sebaceous glands, hair follicles, and arrector pili muscles that contain stem cells and have substantial regenerative potential. The fibroblasts found in the dermis facilitate wound contraction during healing and produce collagen, elastin, and ground substance. Epithelialization of cutaneous defects occurs from wound edges and the basement membrane along hair follicles and adnexal structures. Blood supply derives from both a deep subdermal plexus and a superficial plexus that supplies the superficial dermal papillae.
The skin serves a role as both graft and recipient in most cases of reconstruction. There are a variety of situations where skin grafts are indicated, and grafts are particularly useful for resurfacing superficial defects. Full-thickness skin grafts are also helpful in young patients who have tight skin and sizable defects that are not readily amenable to adjacent tissue transfer. Although skin grafts often minimize the need for additional facial skin incisions, they are susceptible to developing a “patchlike” appearance due to mismatch of color, contour, or texture if not carefully planned. Because of such concerns, skin grafts are used judiciously, proving especially useful in cases that cannot be reconstructed with a local flap or where major distortion would ensue. With thoughtful application of the principles presented herein, many patients can benefit from these aesthetic approaches. As evidence-based approaches evolve in facial plastics, grafting practices should become more consistent so as to achieve optimal outcomes.
Skin grafts may be harvested as full-thickness, split-thickness, or composite grafts with or without hair-bearing skin. The viability of the graft depends on the vascular supply to the recipient bed, thickness of the graft, appropriate compression of graft to recipient site, and patient factors, such as smoking, hypoxemia, diabetes, radiation, and history of prior surgery at the site. Exposed bone, tendon, and cartilage all decrease the probability of successful graft survival. Some irregularity at the junction of skin grafts and surrounding skin is common. When patients are routinely counseled preoperatively regarding the potential role for postoperative dermabrasion or other similar refinements, there is greater acceptance of procedures to achieve optimal match and camouflage of the reconstruction.
Recipient bed preparation
Several technical refinements may improve skin grafting outcomes. Meticulous attention to sterile technique is crucial, because infection greatly increases the likelihood of graft loss. Free grafts are particularly vulnerable to infection, because they do not carry their own blood supply. A variety of approaches may be used for bolstering, including conventional tie-down bolster, quilting sutures, and use of custom contoured compressive dressing. Nobecutane spray may also be used as a transparent antibacterial dressing that is gradually shed. Regardless of dressing, the goal is to minimize shearing forces that may otherwise disrupt vascular connections forming between the graft and the recipient bed. Smoking cessation is also strongly encouraged as tobacco products significantly impair the survival of skin grafts.
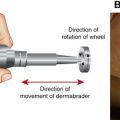
In cases of exposed bone, the likelihood of skin graft survival can be improved by decorticating a thin layer of bone until punctuate bleeding is achieved. If using powered instrumentation, such as a diamond fraise burr, care must be taken to avoid inadvertently cauterizing the perforating nutrient vessels with heat/friction from the burr. Alternatively, holes can be drilled in the outer bone table to access the inner diploë. In cases of extensive bony loss, a muscle flap may be required before grafting. A similar approach may also be useful when grafting on ear cartilage without perichondrium by making windows in the native auricular cartilage. For deeper wounds, it is often helpful to delay skin grafting for roughly 2 weeks, until such time as granulation tissue has formed within the wound bed. The epithelium is then removed before grafting. To decrease bacterial load in granulating tissue, some authors advocate prophylactic use of antistaphylococcal antibiotic beginning 72 hours before skin grafting.
As in other approaches to facial reconstruction, the surgeon should consider facial aesthetic regions and surrounding anatomic landmarks. Marking out the borders of aesthetic units may help ensure preservation of natural facial contours and boundaries. Before skin grafting, defects may be conservatively enlarged to facilitate resurfacing of an entire aesthetic unit. The wound should be of uniform depth, and the edges should be freshened. In contrast to local flap reconstruction, where incisions are oriented 90°, in skin grafting it is often advantageous to maintain a gradual beveled contour transitioning between the skin graft and adjacent facial skin. Risk of trapdoor deformity can often be decreased by developing more acute (rather than rounded) angles in midface reconstruction.
Full-thickness skin grafts technique
Full-thickness skin grafts consist of epidermis and full-thickness dermis, and they are harvested by incising down to subcutaneous fat. In instances where the graft donor site is thicker than the recipient site, judicious thinning to match thickness of skin in the recipient bed may be performed. Conversely, in cases where the defect depth exceeds graft thickness, a small underlay vascular flap or small amount of adipose may be included to increase graft bulk, albeit with attendant decreased risk of take. Full-thickness grafts offer several advantages over split-thickness grafts, including decreased susceptibility to contraction, improved pigmentation and texture match, as well as additional thickness for deeper defects. Despite these advantages, full-thickness grafts nonetheless still contract 10% to 15% on average. Patients are administered preoperative intravenous antibiotics, usually consisting of 2 g cefazolin or 900 mg clindamycin, if penicillin allergic. Patients receive local anesthesia (1% lidocaine with 1: 100,000 concentration of epinephrine) with or without intravenous sedation. The wound and donor sites are prepared sterilely with povidone-iodine. The 45° bevel of the saucerized defect is preserved to facilitate a smooth transition between graft and surrounding skin, thereby avoiding a step-off contour deformity. The template is made of the defect, and the graft is designed slightly larger to accommodate for graft contraction. Subcutaneous tissue is removed from the graft with curved iris scissors.
Because grafts survive initially by diffusion of nutrients (imbibition), the wound bed is optimized by removing eschar, nonvital tissue, or desiccated clot. Ideally, pinpoint bleeding is apparent along the defect, which is readily controlled with pressure and/or topical epinephrine. The graft is secured into position, often incorporating tacking or quilting sutures that help the graft adhere to the underlying tissue. Graft edges are secured with simple interrupted 5-0 chromic sutures. A variety of approaches may be used to compress the graft flush to the underlying recipient bed. A bolster dressing may be made from nonadherent bandage with petroleum-based ointment. Alternatively, cotton balls covered with antibiotic ointment may be wrapped with petrolatum 3% bismuth tribromophenate (Xeroform). Larger bolsters are secured with silk sutures. For small irregular sites, such as the nasal tip or alar margin, it may be most effective to dress the wound and then provide compression with a thermoplast splint sculpted to the shape of the patient’s nose. This custom bolster can then be secured to the surrounding skin with 5-0 Prolene sutures. Bolsters are left in place for 5 to 7 days. If the graft has adhered well to the recipient site, the patient is allowed to get the area wet and cleanse gently. With appropriate bolstering technique, complete graft loss is quite rare. In some cases, a graft may appear cyanotic due to a thin layer of blood deep to the graft or because of hyperemia.
Nasal defects are common sites for skin grafting. As shown in Fig. 1 , skin grafts can achieve excellent aesthetic resurfacing of superficial defects. Skin grafts largely avert the risk of alar distortion that may occur when such defects are reconstructed with bilobe flap or other local flaps. Skin grafts can also provide favorable reconstruction of nasal tip/supratip, in cases where the underlying cartilage topography allows resurfacing with skin graft to restore nasal contours ( Fig. 2 ). In reconstructing nasal tip defects, maintaining profile and avoiding depressed scars are critical; therefore, the surgeon must ensure appropriate graft thickness and adequate soft tissue volume in the recipient bed ( Fig. 3 ). Granulation may be helpful in individuals with thick skin, in whom risk of depressed scar is anticipated. As Fig. 4 demonstrates, even several small defects can be inconspicuously repaired with skin grafting, obviating a 2-staged flap reconstruction procedure while preserving aesthetic units.
Because skin grafts tend to assume the shape and contour of the underlying tissues, they are highly adaptable, allowing effective reconstruction to concave, convex, and planar surfaces. The ear is a common site for skin cancer, and it has many irregular contours. As a result, if often heals favorably with skin grafting, provided adequate perichondrium is preserved ( Fig. 5 ). Skin grafts naturally conform to concave locations, such as the medial canthus ( Fig. 6 ), alar-facial sulcus ( Fig. 7 ), and supra-alar crease ( Fig. 8 ). Tacking sutures are often helpful in preserving creases and junctions. Skin grafts also camouflage planar defects, such as the nasal sidewall ( Fig. 9 ), and provide effective resurfacing for the fine skin found in the eyelids ( Fig. 10 ) and the nasal infratip lobule.