Paramedian forehead and melolabial flaps are the most common examples of interpolated flaps used by facial plastic surgeons and are excellent options for reconstruction of the midface after Mohs surgery. They provide superior tissue match in terms of thickness, texture, and color, while leaving minimal defects at the tissue donor sites. The main advantage of interpolated flaps is the robust blood supply, which can be either axial of randomly based, and the maintenance of the integrity of facial landmarks. The main disadvantage is the frequent need for a multistage procedure, which eliminates some patients from consideration.
Key points
- •
Interpolated flaps are designed from noncontiguous donor tissue, which is based on an axial or random blood supply with the pedicle passing under or, typically, over normal tissue.
- •
Interpolated flaps often require multistaged procedures with pedicle division typically performed at 3 weeks once neovascularization between the recipient and transposed tissue has occurred. Longer intervals between procedures are advised for patients with comorbidities that delay wound healing.
- •
Paramedian forehead flaps are an excellent option for reconstruction of the nasal dorsum with an axial blood supply based on the supratrochlear artery.
- •
The melolabial flap provides an aesthetic advantage to the reconstruction of the lateral nasal sidewall and ala due its preservation of the alar-facial sulcus and minimal distortion of the melolabial crease.
Introduction: interpolated flaps
Due to excellent reliability, vascularity, and skin color match, interpolated flaps are a valuable method for reconstruction of the midface following Mohs surgery. Interpolated flaps are designed from noncontiguous donor tissue, which is based on an axial or random blood supply. Therefore, the pedicle must pass under or, more commonly, over the intervening tissue. The overlying pedicle must typically be removed in a second stage after vascularity is established between the wound and the flap. Therefore, most interpolated flaps are performed in 2 stages. The first stage leaves a temporary bridge of vascularized tissue across normal adjacent skin and the second involves detachment of the flap pedicle after neovascularization from the recipient bed. It is this second stage requirement that is the greatest disadvantage of these flaps. Despite this, however, flaps such as the paramedian forehead and melolabial remain a popular technique when insufficient tissue or mobility in nearby skin prevents coverage of a surgical defect with primary closure or an adjacent flap.
Paramedian Forehead Flap
The paramedian forehead flap (PFF) serves as the workhorse flap for modern reconstruction of large, complex defects. Providing a superior match for nasal skin texture, color, and thickness, the ability of the PFF to reconstruct defects involving more than one layer has made it a classic choice for complex nasal reconstruction. However, the robust vascular supply, the ability to vary thickness of the design, and the ability to provide a large amount of tissue allow for reconstruction of multiple areas of the midface. Defects of the medial canthal region, upper and lower eyelids, medial cheek, nasolabial region, and upper lip may all be reconstructed with a properly designed PFF.
History
The PFF has been used with a variety of modifications since at least 3000 bc . Initially, the primary design was based on the midline forehead involving the central forehead and glabellar skin, resulting in significant donor site deformity. However, in the late nineteenth and early part of the twentieth century, variations were introduced that altered the flap to the median position. Labat modified the median forehead flap to base it on a unilateral supratrochlear artery. Millard is credited with the shift to the paramedian design which excluded the central glabellar skin, subsequently eliminating a significant source of morbidity.
Anatomy and Blood Supply
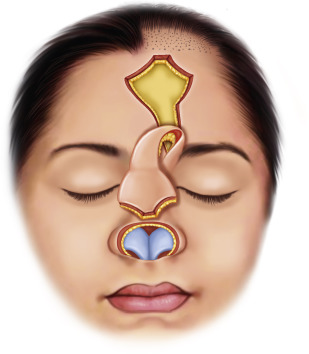
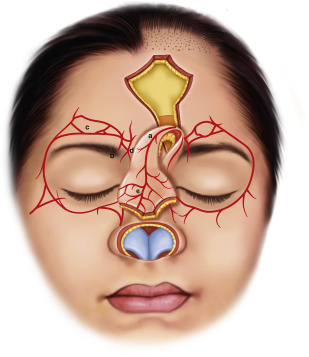
The PFF is clearly thicker than the original skin of the nose due to the unique composition of skin, subcutaneous tissue, frontalis muscle, and thin areolar tissue. Knowledge of the donor area anatomy is, therefore, essential because it allows thinning of the flap for better inset, as well as narrowing of the base of the flap for improved rotation without limiting the overall size of the flap. The primary blood supply of the PFF is the supratrochlear artery. This vessel runs in the submuscular plane, passing deep to the orbicularis oculi muscle and ascending superficial to the corrugator supercilii muscle approximately 1 cm above the brow. There are also important vascular anastomoses from branches of the angular and supraorbital arteries, as well as the medial forehead branch of the dorsal nasal artery. The distal end of the flap is considered a random blood supply that allows for variation in design and preservation of vascularity well beyond the distal end of the axial vessel. It is this excellent vascularity that allows incorporation of cartilage or tissue grafts into the flap. These grafts can, in turn, serve as support or lining tissue in nasal reconstruction. Fig. 1 is an illustration of a PFF used to reconstruct the nasal tip and Fig. 2 illustrates the vascular supply of the flap. Figs. 3 and 4 demonstrate intraoperative PFF reconstructive photos for nasal tip defects.


Design and Technique
The design of the PFF is based on the course of the supratrochlear vascular pedicle. For lateral nasal defects, the flap is generally based on the contralateral pedicle to avoid kinking of the vessels and for maximum rotation and length. Doppler may be used to confirm the location of the vessel. However, cadaver studies show that the supratrochlear artery reliably exits the orbit 1.7 to 2.2 cm from the midline. Taking this into account, the stalk of the flap may be designed to reliably include the supratrochlear pedicle without the use of Doppler, by making the vertical incisions at 1.5 and 2.5 cm from midline. The corrugator complex and frontalis muscles may also be incorporated into the base of the stalk, a technique that is advocated by some investigators to further ensure flap viability.
The use of a foil or paper template is useful to match the defect to the proposed forehead flap. While confirming adequate length required to reach the defect in a tension-free manner, keep in mind the need to include a small amount of extra length to allow for flap thickness and swelling. The random nature of the distal portion of the flap lends itself to variety of designs without compromising blood supply to that area. By extending the PFF superiorly into the hairline or by creating a flap that courses across the midline, the flap may be extended to reconstruct the lower nose and columella. Similarly, for full-thickness defects that involve the intranasal lining, the PFF can be folded over to close the intranasal defect as an alternative to full-thickness skin grafting or a mucosal flap.
Local anesthetic is injected along the periphery of the pedicle to aid in hemostasis while avoiding the supratrochlear vessels. The distal flap is then elevated in the subcutaneous plane from the underlying frontalis musculature, leaving 1 to 3 mm of subcutaneous fat on the underside of the flap. Maintaining the thinness of the flap distally avoids bulkiness and allows a more natural appearance of the flap after inset. As dissection proceeds proximally, the flap is then harvested in progressively deeper layers to preserve the supratrochlear vessels and nerves. After raising the portion for inset, dissection proceeds in the subgaleal plane to preserve the underlying periosteum. Three centimeters above the supraorbital rim the periosteum is incised, and elevation continues in the subperiosteal layer to preserve the periosteal branch of the supratrochlear artery, which supplies additional perforators to the flap. This periosteal incorporation does not decrease the rotational freedom of the flap when using the contralateral forehead, nor does it deter flap length. It does, however, aid in supporting the base of the flap and preventing excessive pedicle torque.
Extending 7 mm above the supraorbital rim, the supraorbital plexus, composed of the supratrochlear, supraorbital, and dorsal nasal artery, provides additional perfusion to the PFF. In higher risk patients, such as smokers or those with poorly controlled diabetes, maintaining this plexus maximizes flap perfusion with a 3-vessel blood supply to the PFF. Conversely, extending the design below the orbital rim allows for maximal rotation. The flap is then rotated and sutured into position.
To close the primary defect, wide undermining is performed. For wider defects, further laxity is achieved by performing galeotomies incised parallel to the skin margins. The wound is then closed in a layered fashion. Although most of the donor site may be closed primarily, often the distal aspect is too wide and under too much tension to close primarily. This portion of the donor site may be allowed to heal by secondary intention with excellent results and minimal scarring. Alternatively, a full-thickness skin graft may be harvested from the postauricular area, or the surgeon may consider a W-plasty closure along the frontal hairline with bilateral advancement flaps.
If necessary, tissue expansion can be performed secondarily after nasal reconstruction to close the donor site or to allow for forehead scar revision. Tissue expanders should be avoided before PFF harvest, however, due to the potential for the reconstructed area to contract after completion of nasal reconstruction.
Detachment
Once neovascularization between the recipient and the transposed tissue has occurred, the pedicle may be safely divided and inset. This has typically been performed at 3 weeks, with longer periods added for patients in whom impaired healing is expected, such as those with poorly controlled diabetes, vasculopathies, or a history of smoking. Klingenstrom and Nylen remarkably performed flaps on themselves to determine the optimal time for flap takedown and published their findings. However, other studies have been performed to establish the appropriate time for takedown of forehead flaps using more objective techniques. More than 3 decades ago, Gatti and colleagues used fiberoptic perfusion fluorometry to measure tissue fluorescence, examining tissue in an animal model at various times after flap transposition and demonstrating that vascular ingrowth begins in the first few days. More recently, Woodard and Most prospectively found evidence of vascular in-growth 1 week following transfer. In a later study, Surowitz and Most demonstrated adequate vascular perfusion by 2 weeks in non-nicotine users using the same technology. Additionally, these investigators suggest that real-time imaging with this system can also be used to identify the origin and course of the supratrochlear artery preoperatively, as well as provide guidance for timing of flap transfer in high-risk patients.
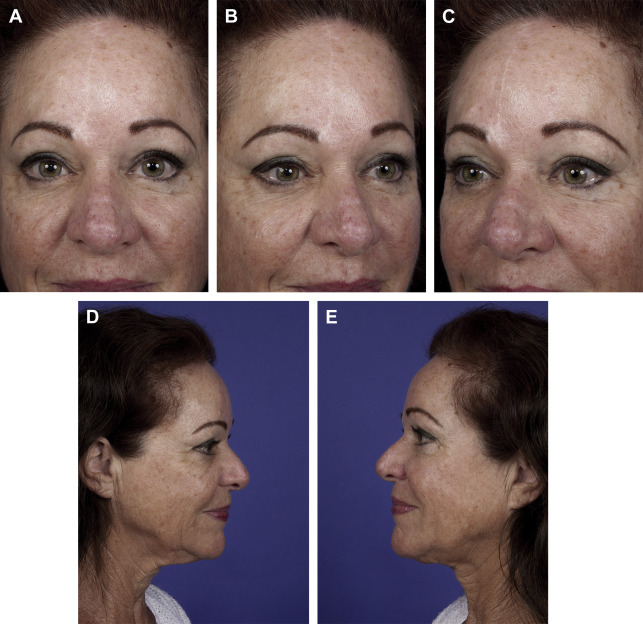
The flap pedicle is taken down by incising the superior portion of the flap, in an inverted V. Inferiorly, the flap is amputated near the margin of the defect and inset. If additional sculpting is required, further conservative thinning of the flap may be performed before closure. Fig. 5 demonstrates a female patient years after multistaged right PFF for a dorsum defect after Mohs surgery.
Related posts:
 In Pursuit of Perfection: The Art of Facial Restoration
In Pursuit of Perfection: The Art of Facial Restoration
 Anatomy of the Skin and the Pathogenesis of Nonmelanoma Skin Cancer
Anatomy of the Skin and the Pathogenesis of Nonmelanoma Skin Cancer
 The Physiology and Biomechanics of Skin Flaps
The Physiology and Biomechanics of Skin Flaps
 Scalp and Forehead Defects in the Post-Mohs Surgery Patient
Defect of the Eyelids
Scalp and Forehead Defects in the Post-Mohs Surgery Patient
Defect of the Eyelids
 Scar Revision and Recontouring Post-Mohs Surgery
Scar Revision and Recontouring Post-Mohs Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


