Fig. 62.1
Anterior view of the dissected right forelimb superficial and deep fascia Star indicates the accessory cephalic vein just beneath the deep fascia
Fig. 62.2
Anterior view of the median nerve and accompanying median artery and veins after wide exposure of the field. Muscle is detached and median nerve was isolated. FCR flexor carpi radialis muscle, N nerve
Fig. 62.3
View of the removal of the nerve fascicles from median nerve segment
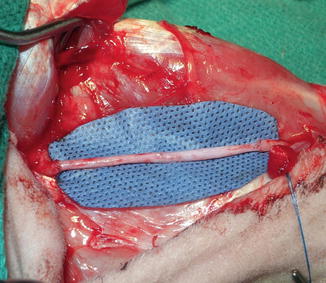
Fig. 62.4
Anterior view of the Epineural sheath conduit after filled with saline
Evaluation Methods
Electrophysiology, histomorphometrical analysis and immunohistochemistry are the commonly used parameters for nerve assessment. Behavioral studies are not applicable for this model because median nerve injury does not produce significant functional deficit [3].
Evaluation of the Nerve Function
Motor nerve conduction studies can be done in certain time points, such as just before the initial nerve surgery, every 3 months and at the end of the study. To record the compound muscle action potential, anode electrode is placed on the hoof palmar skin, the cathode electrode plate on the belly of flexor carpi radialis muscle and the ground plate on the back of the forearm. Then the median nerve can be stimulated with an impulse. Compound motor action potential (CMAP), latency and distance (the length between the recording electrode and stimulator) are measured for further analysis. CMAP amplitude reflects the number of functional axons. In hindlimb, tibialis nerve function can be assessed by measuring gastrocnemius muscle activity.
Six months after nerve repair, each sheep was anesthesized without neuromuscular blockade and the surgical sites were exposed for assessments (Fig. 62.5). Depending on the experimental protocol, this time period can be extended to 9 or 12 months.
Fig. 62.5
 Microcirculation Model for Invasive Animal Monitoring
Microcirculation Model for Invasive Animal Monitoring
 Composite Osseomusculocutaneous Thymus Allotransplantation Model
Composite Osseomusculocutaneous Thymus Allotransplantation Model
 In Vivo Chimera Model: Creation of Primary and Secondary Chimera
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
 Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
 Heterotopic Vascularized Ovarian Autotransplantation Model in the Sheep
Heterotopic Vascularized Ovarian Autotransplantation Model in the Sheep
 Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer




Related posts:
Microcirculation Model for Invasive Animal Monitoring
Composite Osseomusculocutaneous Thymus Allotransplantation Model
In Vivo Chimera Model: Creation of Primary and Secondary Chimera
Experimental Model for Monitoring of Composite Tissue Transplantation Induced Trauma
Heterotopic Vascularized Ovarian Autotransplantation Model in the Sheep
Defect Repairs After Resections of Laryngeal Cancer, Hypopharyngeal Cancer, and Cervical Esophageal Cancer
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
