Key points
- •
Selection of the correct filler for the patient and area to be treated.
- •
Safety in filler selection.
- •
Training in the use of new fillers.
- •
Off label uses of fillers.
- •
Classification of the new fillers.
Introduction
The vast choice in fillers is challenging for both the consumer and the physician. In some parts of the world the filler is produced then marketed and after tremendous use it undergoes randomized testing to see if it actually works and is safe. This reverse cycle has been put in place by the manufacturers and does put all involved at risk. Despite the large numbers the actual complication rates are relatively low. Most often the new fillers are introduced in the market in Europe and then adapted by the USA/Canadian practitioners once the filler is approved by the FDA and Health Canada respectively. This does allow for some prior assessment of the newer filler products and some foresight into their future roles for cosmetic use.
The soft tissue fillers along with the use of botox cosmetic have dramatically changed the approach to facial and body rejuvenation and contouring. This is an area of rapid expansion and has made it very exciting for patients and practitioners. The future fillers are rapidly changing and this chapter will focus on the fillers that will play a role in the market due to their predictable use and unique characteristics. By the time this publication is in print there will be several new fillers and botulinum toxins that will be ready for use in the market place.The new and future fillers are temporary, semi-permanent and permanent types. Some are combined with lidocaine to decrease the discomfort of the injection.
Macrolane ™
Presented at the beginning of 2007 by Per Heden after a pilot study carried out in 2004, Macrolane™ gels are new possibilities for body shaping. These gels are the first to be presented for injection in large volumes in the body. They add volume in an instant and have long-term stability. Like all the Q-Med (Restylane) products, this NASHA gel is an stabilized, biocompatibile and absorbable product. It is available in two formulations, or so called volume restoration factor, Macrolane™ VFR 20 and Macrolane™ VFR 30. Each of these products have been created to restore different levels of tissue support.
The injection depth varies from subcutaneous to subperiosteal depending of the site to be treated. The low VFR 20 (Macrolane™ 20) is adapted for areas of the body with less tissue support to cover, as it can happen in very thin patients, in breast areas for the correction of wrinkling or in abdomen correction with very thin tissue layers. The thicker VFR 30 (Macrolane™ 30) is a thicker gel for the correction of substantial tissue cover, as for example buttock correction or in case of defects of liposuction in thick tissue areas.
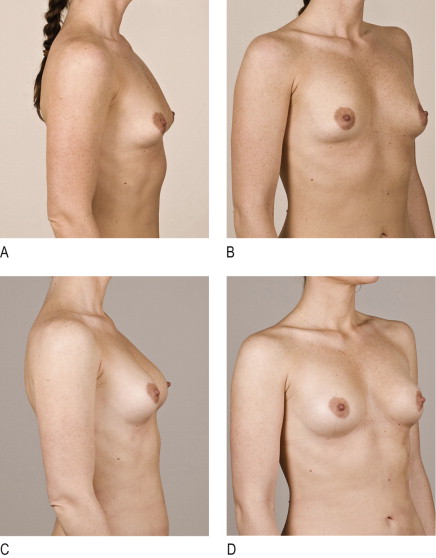
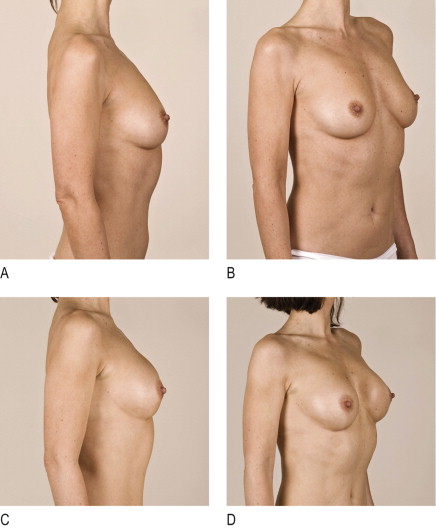
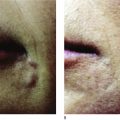
These materials are for physicians experienced with the treatment sites and with a thorough knowledge of techniques like lipofilling, as these gels fill out large areas at deep tissue level with an immediate result ( Figures 10.1, 10.2 ). The indications are corrections of non-facial deformities, such as trauma scars, scarring and atrophy after liposuction, contouring of concave body deformities or enlargement of body areas experimentally including breast augmentation. It should be less invasive than fat transplantation, is absorbable giving long-lasting results and few adverse events (AE). The most common AE is a local inflammation in the case of body restoring, which should resolve within 2 weeks with topical ointments and oral antibiotic therapy. Local symptoms such as redness, edema and pain are common to most facial fillers. With Macrolane™ migration has been seen and in the breast pilot study, where amounts of 100 ml of gel were used, microcalcifications with radiological research.
Patient selection
Most of our patients are searching for non-invasive aesthetic treatments, with low risk and no scarring. Furthermore, they desire no general anesthesia risk or recovery time but a perfect long-lasting result. Additionally, there are patients who fear surgery but desire immediate results, low complication rates and acceptance from friends and family. A good candidate should comprehend the limits of the material, being absorbable and limited in the quantity to be injected, around 100–120 ml per area.
Technique
The injections should be performed under local anesthesia, if the area to be corrected is not too large. The physical area where the injection is to be administered must respect specific terms of tissue cover and skin excess. These must be measured before the treatment with a stretch-test and a pinch-test.
Stretch test
To determine if there is skin excess and therefore no Macrolane™ indication, mark two points at the edge of the area to be treated. Stretch than this area and remeasure the new distance with a calliper. In the case of a distance augmentation of over 50%, the patient should not be treated because of the excessive skin laxity.
Pinch test
Pinching a double fold of tissue at the border of the area to be treated the fold should measure over 2 cm.
Injection technique
The injection technique is similar to the traditional fat transplantation. In case of local anesthesia avoid excessive liquids or tumescent techniques, as these may distort the area to be treated. A small incision (blade 11) at the edge of the area to be treated gives access to a blunt 0.2 cannula mounted on the 10 ml syringe of Macrolane™. The tip is then introduced in the fatty subcutaneous tissue or subperiosteally, and moving back and forth the material is delivered in small doses without extensive pressure. Overcorrection should be avoided, and leakage of material from the injection site also. Post-treatment is a light massage, ice on the treated area and local antibiotic ointment. Immediately post-op, the patient should avoid exercising or any kind of activity that could cause pressure on the treated area.
The manufacturer (Q-Med) described that the results should last up to 1 year. The question is whether costs cover the result, but many patients, after experience of good aesthetic results, shift over to cosmetic surgery. The cost may be up to £10 000. There is no publication of breast augmentation. On 16–18 May 2008, Dr Giovanni Botti, the breast guru from Italy, gave the first public presentation of Macrolane™ with the possibility of obtaining certification to use Macrolane™ for the body. Officially, it is not allowed for pure breast augmentation, only for correction of wrinkling or retractions or asymmetries. In a recent article in Bazaar magazine in the UK, the editor underwent the treatment with Dr Chris Inglefield, reported on the procedure and is delighted with the results. It has been used in Japan for 3 years with good follow-up of 1100 patients with high levels of satisfaction.
Restylane Lipp ™
Restylane Lipp™, which is smooth and extensible, is the first filler created specifically for mucosal and submucosal enhancement. In the past few years, many lip augmentations have had variable aesthetic results, resulting most of the time in visible, static, tense and unnatural aspects. The inferior third of the face is dominated by the lip, and a good shape and fullness are desired, giving a youthful look. With aging the lips lose volume and fullness, they become flat and subtle, and inverted by a longer nasolabial distance and hypotonic muscles. Restylane Lipp™, the new Q-Med NASHA, has a compact/cohesive gel and gives a natural looking correction of the lip.
The treatment aims to define the shape, to correct volume loss and to enhance the vertical projection of the lips. The treatment needs a higher artistic sense than only a wrinkle correction, avoiding excessive volume replacement. The compact/cohesive gel has been created for the specific lip anatomy. The submucosal layer is different from the subcutaneous layer, and any correction material must be able to penetrate homogenously in the intercellular matrix. Restylane Lipp™ is a dynamic gel able to support the intrinsic lip movements giving them a smooth and sensual aspect.
Patient selection
Understanding lip anatomy and the aesthetic ratios is essential for optimum lip augmentation. It’s not a linear structure but presents different contours, volumes and inflections. In a youthful lip the ideal ratio of the upper to the lower lip is 0.6–1. Asymmetries are nearly always present, and should be identified and pointed out prior to the treatment. The basic issues in augmentation are the vermilion border, oral commissure elevation, volume replacement and vertical rhytides. Restylane Lipp™ is only indicated for volume restoration resulting in cohesive skin corrections.
The patient should be informed as with every filler treatment, but especially of the common effects like redness, edema, tension and ecchymosis after the augmentation. They also should know that touch ups are frequently necessary, as overcorrection with this thick gel must be avoided. Vertical skin defects and the oral commisure should be corrected with Restylane®, or with other techniques as laser ablation or peels.
Technique
Regional nerve blocks are very effective in lip augmentation, as the intramucosal infiltration causes pain. The technique is a slow linear injection in the submucosal layer. Holding the syringe parallel to the lip, and giving a light tension stretching the lip with the thumb, the material is injected with the threading technique. The physician must control a very equal distribution of the implant, which needs experience and aesthetic sens. Overcorrection must be avoided, as the material can not be massaged away easily, and breaking the cohesion of the gel by traumatic compression irregularities will show up immediately. For a good lip augmentation, four to six threading injections are sufficient for every lip. The vermilion border should not be corrected with this compact material, but instead with Restylane®. Superficial injections in the mucosa show up with bumps, so should be avoided. Only the submucosal layer should be injected.
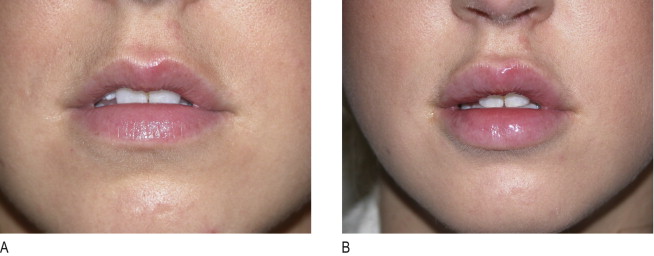
Restylane Lipp™ is a dynamic cohesive gel for volume restoration of the lip, for expert hands with a good aesthetic sense. The compact gel is optimum for the intercellular lip matrix, adapted to the continuous intrinsic labial massage, and gives long-lasting results of 1 year or more ( Figures 10.3, 10.4, 10.5 ).

Related posts:
 Third generation polymethylmethacrylate (PMMA) aesthetic soft tissue fillers for the correction of nasolabial folds and other applications
Third generation polymethylmethacrylate (PMMA) aesthetic soft tissue fillers for the correction of nasolabial folds and other applications
 Injectable silicone: current role
Injectable silicone: current role
 Poly -l-lactic acid (Sculptra®)
Poly -l-lactic acid (Sculptra®)
 Periorbital rejuvenation with injectable fillers
Periorbital rejuvenation with injectable fillers
 Avoidance and treatment of complications after dermal filler injections
Avoidance and treatment of complications after dermal filler injections
 Possible causes and treatment options of dermal filler granulomas
Possible causes and treatment options of dermal filler granulomas
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


