Key points
- •
Permanent filler.
- •
Not all PMMA fillers are manufactured the same and may therefore have different complication rates.
- •
Technique is critical with permanent fillers.
- •
Best applications are nasolabial folds (FDA approved), nasal defects post-rhinoplasty (off-label), marionette lines (off-label), corners of the mouth (off-label) and radial wrinkle lines of lips (off-label).
- •
Most complications can be treated by intralesional steroid injections or simple removal.
Polymethylmethacrylate (PMMA) implants have been used in various formulations for many years throughout the world and more recently were FDA approved in the United States as a third generation implant (TG PMMA), ArteFill®. The TG PMMA, ArteFill®, was manufactured by Artes Medical Inc. based in San Diego, California until the fourth quarter of 2008 when the company declared bankruptcy. Worldwide, PMMA implants continue to be one of the leading permanent dermal fillers and because of the comprehensive nature of the FDA study, which included 5-year follow-up detail, the information presented in this chapter should benefit the reader contemplating using PMMA devices. In today’s ever-changing business world, it is also conceivable that the TG PMMA, which may indeed be the gold standard of PMMA products, will be resuscitated and re-appear in the US market. Herein, the history of PMMA implants is discussed with a focus on the TG PMMA. Please note that the original FDA submission was based on data derived from use of Artecoll®, a second generation PMMA, which is still in common use in Europe, Asia, Canada and South America.
Introduction
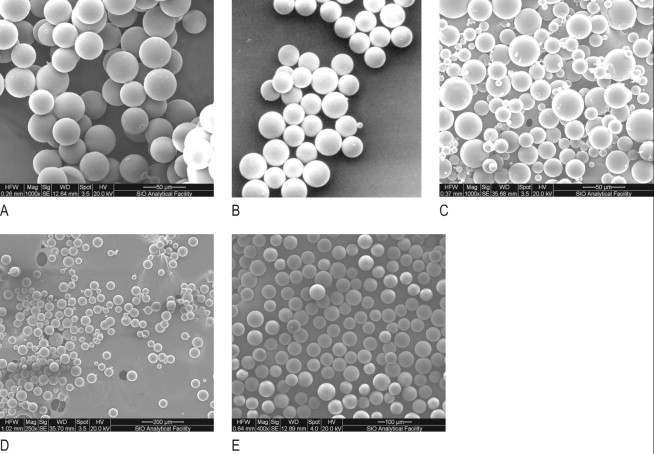
Biological dermal fillers reliably and safely augment facial wrinkles and folds, but necessitate repeat treatments after they have been resorbed, generally within a 12 month period ( ). TG PMMA, a novel permanent implant, was developed as a permanent implant to overcome this limitation. This soft tissue filler is composed of polymethylmethacrylate (PMMA) microspheres suspended in a collagen gel matrix containing 0.3% lidocaine. It is a third generation PMMA based filler product that contains an optimized collagen matrix with microspheres which have enhanced uniformity and consistency as well as near elimination of nanoparticles compared to the second generation PMMA product Artecoll® and the original formulation, Arteplast®. This is a critical distinction as not all PMMA products are the same and scanning electron microscopy can show a wide variation of nanoparticles, sphere irregularities and sphere shapes and sizes, all of which might contribute to early or late adverse events ( ) ( Figure 3.1 ).
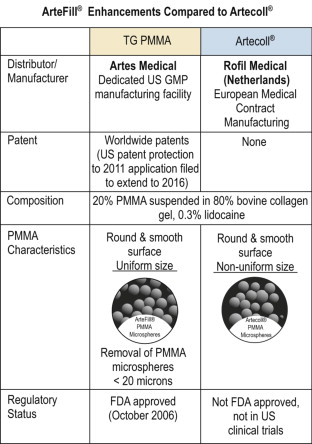
TG PMMA has been approved by the FDA for the correction of nasolabial folds, based upon results of a US pivotal trial with the second generation predecessor product, Artecoll. Since the initiation of the pivotal trial, substantial improvements in the second generation PMMA product have been made, resulting in a newer generation of product ( Figure 3.2 ). Refinements in manufacturing have increased the uniformity in the size of the microspheres. The proportion of particles which are less than 20 microns in diameter has been reduced to <1%, and in fact, are typically non-detectable in the finished product. These manufacturing changes, made in cooperation with the FDA, are believed to have further improved the tolerability of the implant as smaller particle size elements (e.g. < 20 microns) are thought to promote phagocytosis ( ). The product was manufactured in the US using bovine collagen sourced from a restricted closed herd in the US. For simplicity, in the balance of this publication the product will be referred to as the PMMA filler, unless otherwise noted.
The pivotal trial was a randomized, double-blind, controlled study involving 251 men and women, comparing this novel PMMA filler (n = 128) to a collagen control filler (Zyderm® II or Zyplast®, n = 123). Efficacy was determined using a six-point Facial Fold Assessment (FFA) photometric validated grading scale ( ). This scale was used for masked observers’ assessments of standardized photographs in which the mean score of three independent graders was designated as the primary efficacy measure. This same scale was also used for investigator nasolabial fold grading (secondary efficacy measure).
In this pivotal study, the subjects receiving the PMMA filler exhibited significant nasolabial fold correction, superior to that of the collagen control at both three and six months post-injection (P < 0.001, for both primary and secondary efficacy measures). The superiority of the PMMA filler was observed despite the fact that a substantially smaller quantity of material was utilized than in collagen control cases (0.82 vs 1.46 cc/fold, P < 0.001). The effect of the collagen control treatment virtually disappeared by six months. Nonetheless, in comparison to baseline (prior to any treatment) the PMMA filler demonstrated significant nasolabial fold correction at 12 months (P < 0.001, for both primary and secondary measures). To further substantiate the durability of this novel implant material, a long-term 5-year follow-up safety and efficacy study based upon subjects enrolled in the original pivotal study was performed.
Summary of 5-year study: materials and methods
This is a long-term follow-up study of PMMA filler treated subjects who participated in the original multi-center pivotal study ( , ). The same methodology used in the pivotal trial to substantiate the safety and efficacy of the product was applied to evaluate the product in subjects 5 years after their last treatment. The primary objective of the study was to determine efficacy for nasolabial folds based upon masked-observers’ FFA evaluations, and safety using unanticipated event assessments. Secondary objectives were to evaluate efficacy by means of investigators’ FFA evaluations, investigators’ success ratings, patients’ satisfaction ratings, and masked observers’ FFA for 5 years versus 6 months. All of the investigators (eight US sites) involved in the original pivotal trial participated in the study.
Study candidates included those subjects initially randomized to be treated with the PMMA filler (n = 128) plus the subjects in the collagen control group who had elected to crossover to the PMMA filler therapy at the conclusion of their 6-month collagen control treatment period (n = 106), for a total of 234 potential subjects. On or about the 5 year anniversary date from their last treatment, each investigator contacted their PMMA filler subject(s) by telephone and/or certified letter and encouraged them to be enrolled in the trial.
All subjects were asked to participate in a single follow up visit. At this visit the following tasks were performed: investigator clinical grading (FFA scale and clinical success), facial photographs (for masked-observer assessments), subjects’ ratings of satisfaction, recorded adverse events and the documentation of any additional facial aesthetic procedures that had occurred since the last PMMA filler treatment. Investigators judged whether the additional aesthetic treatments had a possible or probable impact on effect of the novel PMMA filler’s correction. Nasolabial folds were considered possibly affected by an intervening facial aesthetic treatment if it occurred in the same region as the PMMA filler injection or if it were applied to the entire face. Nasolabial folds were considered to be probably affected by an intervening facial aesthetic treatment if it affected the area of correction achieved by the PMMA filler injections. For all participating sites, the 5-year follow up study protocol and associated consent was reviewed and approved by a central Institutional Review Board.
Assessment of nasolabial folds was based upon grading using the Facial Fold Assessment (FFA) grading scale. The FFA scale is a validated six-point, photometric index of the severity of nasolabial folds, ranging from 0 (none) to 5 (severe) ( ). The primary efficacy variable for this study was based upon the review of standardized subject facial photographs using this measure. Photographs of patients were taken using the same photography system and processed by the same film laboratory as in the pivotal trial. To minimize grader biases, photos from the pivotal study 6-month time point as well as the 5-year time point for each enrolled subject were evaluated. The photographs were provided to three independent masked observers (board-certified dermatologist or plastic surgeon) in random order, to be evaluated during the same session using the FFA scale. The observers were masked with respect to time point and treatment of the patients in the photographs. The subject’s facial fold severity score was then determined based upon the average of their three independent evaluations using the FFA scale. In the case of bilateral treatments, the ratings for the two sides were averaged. The change from pretreatment to six months was computed using the original set of 6-month photograph ratings. Change from 6 months to 5 years was computed using the new set of 6-month photograph ratings. Finally, the cumulative improvement over the 5-year interval was computed as the sum of these two changes. This technique avoided any potential bias due to rater drift in the analyses. This FFA grading scale was also used by the investigator to clinically grade each subject’s nasolabial folds as a secondary measure of correction.
Ratings of success and satisfaction
In addition to assessing the degree of nasolabial fold correction using the FFA scale, other methods were used to evaluate cosmetic correction. A five-point ordinal scale was used by the investigators to rate the success of treatment with the novel PMMA filler, ranging from ‘not at all successful’ to ‘completely successful’. Likewise, subjects rated their satisfaction with the PMMA filler according to a similar five-point scale ranging from ‘very dissatisfied’ to ‘very satisfied’ ( Table 3.1 ).
| Investigator success scale |
|
| Patient satisfaction scale |
|
Statistics
Efficacy data were analyzed for normal distribution by the Kolmogorov-Smirnov test. Paired t-tests were employed unless distributions were found to deviate significantly from normality, in which case the Wilcoxon matched-pairs signed-ranks test was used. Other statistical tests are identified individually in the Results section.
Results
Patient demographics and response rates
From the original pivotal study subject pool, 145 patients responded (145/234 or 62%). Three subjects, however, were excluded from the efficacy analysis because their long-term follow–up period was less than 4.5 years. Of the remaining 142 subjects, 15 were males and 127 females (mean age 52.4 years), 82 subjects were from the original TG PMMA group (64.1%) and 60 subjects in the crossover group (56.6%), with a mean follow up period of 5.36 years (range 4.53 years to 6.32 years) after their final treatment with the PMMA filler. Comparison of the original PMMA filler and crossover groups revealed no significant difference in terms of follow-up rates (chi-square, P = 0.245).
During the pivotal trial, this PMMA filler had been used to treat a variety of other anatomic sites (e.g. glabellar folds, mouth corners, etc.). In this follow up report, however, the focus was limited to the FDA approved indication only; the treatment of nasolabial folds. In this group of 5-year follow-up subjects, 124 had nasolabial fold correction; most treatments were bilateral, one was unilateral. These subjects provided the basis for the efficacy evaluation.
Masked observer facial fold assessment ratings of efficacy at 5 years compared to baseline
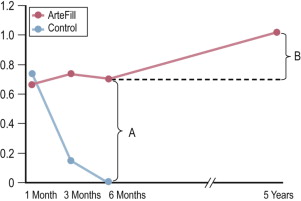
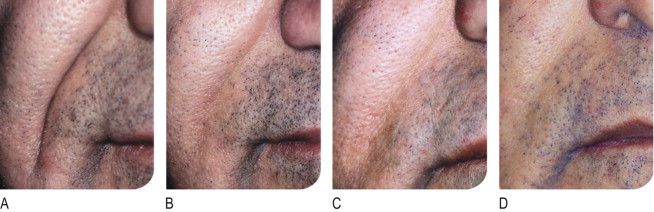
The PMMA filler maintained significant cosmetic correction in nasolabial folds at 5 years after their last treatment compared to baseline (n = 119). Five of the 124 nasolabial fold subjects were excluded from this analysis because they did not have either baseline or 5-year photographs. Figure 3.3 shows an improvement of 1.01 points in masked observer FFA for this time period (P < 0.001, paired t-test). Given that the FFA is a 0–5 scale, a change of one point represents a substantial improvement in cosmetic effect. Actual results are illustrated in photographs of a male ( Figure 3.4 ) and female patient ( Figure 3.5 ). Before treatment (baseline), the male patient exhibited a pronounced nasolabial fold, which was dramatically improved by 6 months and continued to improve at 12 months and 5 years. The inter-rater agreement for nasolabial folds was found to be high (intraclass correlation coefficient = 0.845).
Secondary measures of efficacy at 5 years compared to baseline
Secondary efficacy measures also revealed favorable findings for the durability of the PMMA filler. Investigator FFA scores significantly improved at five years compared to baseline, by 1.67 points (n = 122, P < 0.001, paired t-test). These results were consistent with the five-year success rated by investigators (90% described the cosmetic effect as ‘completely successful’ or ‘very successful’, n = 123) and satisfaction by the patients (90% described themselves as ‘very satisfied’ or ‘satisfied’ with the cosmetic outcome, n = 123) ( Figure 3.5 ).
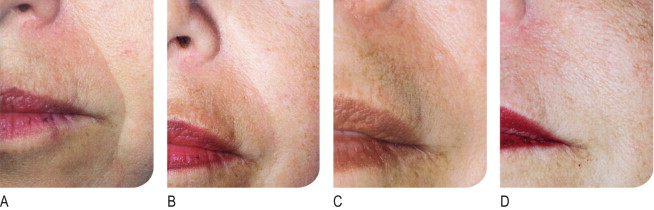
Efficacy at 5 years compared to 6 months
The PMMA filler not only maintained nasolabial fold augmentation between baseline and 5 years, it also improved masked observer FFA ratings by 0.20 points for the time period between 6 months and 5 years ( Figure 3.3 , item B), indicating that the cosmetic effect improved gradually but significantly (P = 0.002, n = 113, paired t-test). This is evident in the patient photographs, particularly when comparing the one-year and five-year time points ( Figure 3.4 , Figure 3.5 ). In a paired analysis of the group of crossover patients (n = 45), the PMMA filler-induced improvement assessed 5 years after treatment with this novel filler (0.91 points) was significantly greater than the collagen-induced improvement measured at 6 months (0.01 points) as rated by masked observer FFA (P < 0.001, paired t-test).
Potential biases
The authors recognize that bias could potentially arise from a number of sources, including additional cosmetic procedures since the last PMMA filler injection. A total of 58 patients underwent such procedures. When this group was compared to the group that did not receive intervening treatments, no difference was discovered in change in masked observer FFA rating at five years relative to six months (P = 0.516, t-test). In a separate analysis, patients were stratified into three subgroups, according to whether their impact from intervening treatments was possible, probable, or none. In no case did these subgroups differ significantly from each other (one-way analysis of variance). Furthermore, the improvement in masked observer FFA scores from baseline to five years was still evident in patients who had had no impact from additional treatments (P < 0.001, paired t-test).
Efficacy data were also scrutinized for potential bias due to attrition. After stratification of patients into groups with and without follow-up, no significant differences were found in terms of age (P = 0.963, t-test) or gender (P = 0.170, chi-square test). It is, however, important to note that the study subjects did achieve greater improvement at 6 months in contrast to the balance of the original PMMA filler subjects which did not participate in this study, potentially suggesting some selection bias (P = 0.009, t-test). However, when the participating study subjects were divided into two subgroups based on their 6 month findings; low responders (defined as those under 0.8 FFA points improvement) and high responders (defined as those with more than 0.8 FFA points improvement) showed significant improvements in efficacy at 5 years compared to 6 months outcomes (P < 0.044 and P < 0.024, respectively, paired t-tests).
Safety review
In this study, 145 subjects were evaluated for safety; 28 total adverse events were experienced by 21 subjects; and the 20 treatment-related events were distributed among 15 subjects ( Table 3.2 ). Mild treatment-related events occurred in 8.3% of the total population; moderate events were reported in 1.4%, and severe related events in 0.7%. The most common treatment-related adverse event was lumpiness, 80% of which were deemed mild.
Related posts:
 Injectable silicone: current role
Injectable silicone: current role
 Poly -l-lactic acid (Sculptra®)
Poly -l-lactic acid (Sculptra®)
 The potential role of adipose derived stem cells as semi-permanent/permanent fillers in aesthetic surgery
The potential role of adipose derived stem cells as semi-permanent/permanent fillers in aesthetic surgery
 Avoidance and treatment of complications after dermal filler injections
Avoidance and treatment of complications after dermal filler injections
 Possible causes and treatment options of dermal filler granulomas
Possible causes and treatment options of dermal filler granulomas
 Shaping the future: new outcomes in Europe
Shaping the future: new outcomes in Europe
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


