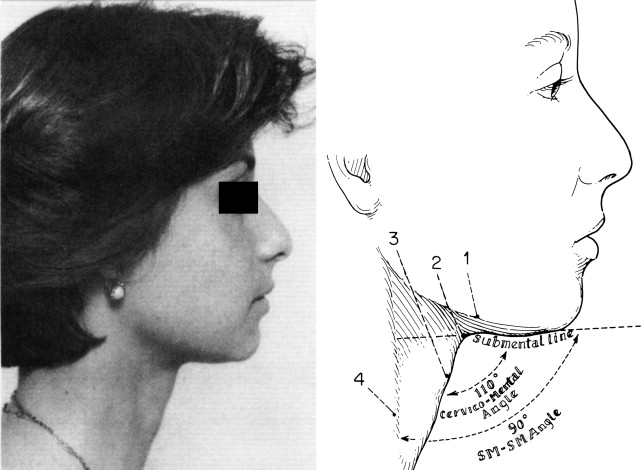
After a visit to Bruce Connell in 1975, I realized I had seen the ultimate answer to neck correction in facelifts—the treatment of the muscles, the removal of fat both superficial and deep, and the skin tightening. I devised a neck-only lift using his principles. These consisted of submental incision, removal of all fat inferior to the mandibular border, closing the platysmas at the midline, cutting the platysma at the level of the hyoid, exercising great care with the proximity to the marginal mandibular nerve, and allowing the natural elasticity of the skin to retract over the new framework.
Key points
- •
By performing a necklift by this technique many pearl size pieces of fat were created. These “pearl fat grafts” were placed in various folds and depression of the face as filler.
- •
The fat removed from the neck was grafted through incisions and tunnels in the face.
- •
Three principals in the technique include removal of fat to the inferior mandibular border, tighten the loose muscle to create a youthful neck and allow the skin to redrape by its own elasticity.
Editor Commentary: It is more than 30 years since Richard Ellenbogen described the essential visual criteria for restoring a youthful neck. I encourage readers to keep these criteria in mind as they read the other articles in this coverage of neck lift. In this article, Richard describes how his technique for rejuvenating the neck has evolved, always setting the goals of a happy patient, a predictable result, and minimizing the risk of complications by keeping it simple.
After a visit to Bruce Connell in 1975, I (Dr Ellenbogen) realized I had seen the ultimate answer to neck correction in facelifts—the treatment of the muscles, the removal of fat both superficial and deep, and the skin tightening. Dr Connell’s patients were older than mine, as a rule, and, as a young plastic surgeon, I devised a neck-only lift using his principles.
These consisted of
- •
Submental incision
- •
Removal of all fat inferior to the mandibular border
- •
Closing the platysmas at the midline
- •
Cutting the platysma at the level of the hyoid
- •
Exercising great care with the proximity to the marginal mandibular nerve, and
- •
Allowing the natural elasticity of the skin to retract over the new framework
Dr Connell had never done the neck at this time as an isolated procedure. When I published in Plastic and Reconstructive Surgery in 1980, I entertained doctors from around the globe, demonstrating the technique for a procedure that I did not think deserved any special recognition because Guerrosantos had already done it.
I had, at the termination of each neck lift, a pile of small pieces of fat removed from the neck and began placing them in tunnels thru the nostril into the nasolabial folds and in the lips and cheekbones. I researched the world’s literature on fat grafting and noted that “pearl fat grafts” were done in the early 1900s. This fat grafting was 7 years before the liposuction task force returned from France. The extraction of fat by cannula was not yet devised in America.
My neck article was published in 1980, 2 years after submission to an academic journal. My rediscovery of fat grafting was submitted 4 times over 4 years to an academic journal and returned with the criticism, “grafted fat doesn’t last.” It was ultimately published in Annals of Plastic Surgery in 1984 after many lectures at various professional societies. Sydney Coleman, while a resident in San Francisco, attended my lecture and spread the word that fat does graft and remain. In the performance of my neck lift, fat grafting was rediscovered serendipitously.
Why is a neck lift like a kiss?
Dr Ruth once said, “When you kiss do you do it to please your partner or please yourself?” A neck lift is very much like this. Of course, the patient must be pleased foremost but many physicians try too hard and use extraneous or possibly unnecessary techniques when possibly not necessary (gland excision, digastric excision, platysma cutting or excision, and postauricular excision).
Another kiss analogy is KISS— k eep i t s imple s tupid. Avoid variations with higher complications and prolonged recovery. My techniques and thousands of neck lifts follow that principle.
Why is a neck lift like a kiss?
Dr Ruth once said, “When you kiss do you do it to please your partner or please yourself?” A neck lift is very much like this. Of course, the patient must be pleased foremost but many physicians try too hard and use extraneous or possibly unnecessary techniques when possibly not necessary (gland excision, digastric excision, platysma cutting or excision, and postauricular excision).
Another kiss analogy is KISS— k eep i t s imple s tupid. Avoid variations with higher complications and prolonged recovery. My techniques and thousands of neck lifts follow that principle.
Surgical approach
My approach, and this is a simplified version of my present approach, was learned after many favorable and less than favorable results
- •
I almost universally use a submental incision of approximately 2–3 cm back from the inferior mandibular border at the midline.
- •
I do not use tumescent anesthesia. It seems to cloud the muscle fat border colors and makes excision or the fat more difficult.
- •
I inject 20 mL of 1/200,000, 0.5% lidocaine, and listen to country music for 20 minutes.
- •
I dissect the fat from the skin and scrupulously remove the fat superficial to the platysma below the inferior mandibular border.
- •
In a fat or heavy neck, I separate the platysmas at the midline and remove subplatysma fat, cauterizing well all bleeders.
- •
I see no reason to ever remove the digastrics. I remove as far as I can posteriorly by direct vision.
- •
I make a small incision behind the earlobe and, with a 3-mm cannula, suction the fat at the angle of the mandible I could not see from the midline incision and liposuction the borders of the fat excision inferiorly to feather all edges.
- •
I close the platysma with buried 4-0 nylon.
- •
I rarely remove an anterior platysma border unless the platysma is flaccid on closure.
- •
I insert a 3-mm suction drain in each postauricular liposuction cannula hole.
- •
The incision under the neck is closed subcuticularly and a light compression dressing is used for 24 hours.
- •
I use a postauricular skin and platysma tightening incision only rarely, when it is obvious that lax skin must be tightened—usually in the older thin neck.
I have simplified the description of my technique that goes along with the simplification of my technique:
- •
I do not resect submandibular gland.
- •
Occasionally, I plicate the platysma over the gland to move it more superiorly.
- •
I never depend on fibrin glue to take the place of meticulous hemostatic surgery.
- •
I rarely use a Giampapa stitch, but I think that it is a good idea, when necessary, to elevate sagging submental structures after platysma closure.
See procedural diagrams and descriptions in Figs. 1–4 .