Key points
- •
Patients often ask for enhancement of breast shape, so the new breast must be controlled dimensionally. The extension must be controlled horizontally, vertically and anteriorly.
- •
Consideration of the new way of approaching a breast augmentation including patient education and information.
- •
Size is less important. Proportion, shape and acceptance of patient limits must be discussed and agreed upon.
- •
Introduction and consideration of a new generation of implants: implant shape, designed to reshape the final breast shape more closely to anatomical shape; and gel consistency to keep the implant shape and to control the soft tissue distribution.
- •
Introduction of a plan to evaluate the patient dimensions and characteristics, select an appropriate implant and plan the surgical technique.
- •
Introduction of new principles and surgical techniques to match the pocket limits and internal soft tissue modification to achieve the best results from the outset.
Introduction
For the past four decades we have primarily been using round, soft, ‘responsive’ silicone gel implants for breast augmentation. Our best attempts however, have often been unsuccessful in producing a long-term, predictable, stable and attractive enhancement of the breast. It is not surprising that in an organ subjected to monthly hormonal changes, pregnancies and fluctuation of body weight, it is difficult to achieve a lifelong attractive and stable result by placing an implant in it as while the implant itself does not change much over time, everything surrounding it does ( ).
During this era, with few implant options to choose from, the only decision that had to be made concerned the size of the implant. While some of our patients had good long-term results, others seemed to deteriorate with time. Silicone gel implants appeared to keep the breasts of some of our patients attractive and rejuvenated but accelerated breast aging in many others. If all patients and breasts were alike and the only change that occurred following insertion of the implant in a breast was making the breast bigger, then issues such as individual tissue and implant characteristics and the dynamics between the two would be irrelevant. The rationale behind the evolution of and the movement towards cohesive, form stable implants was driven by patients and surgeons who were looking for better long-term outcomes. A stable appearance of an augmented breast requires a shape stable device and a stable interaction between the implant and the soft tissue envelope surrounding it.
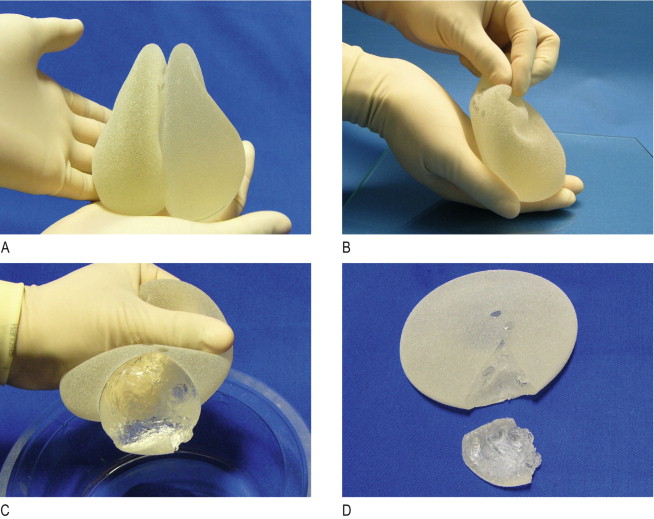
As we cannot prevent hormonal changes and aging from occurring in the breast, we need to establish a predictable relationship with an implant. This means that the implant should fit the breast like a ‘hand in a glove’, have an even, constant distribution of gel throughout the shell in any position and be perfectly filled with cohesive gel so that there are almost no wrinkles on its surface. Form stable implants maintain a constant shape in and outside the breast, and the cohesive gel used to fill them does not spread when broken ( ). The first introduction of anatomical, form stable implant (style 410 FM by McGhan) was in 1994 by Tebbetts. Originally these implants were conceptualized to produce a durable, longer-lasting, wrinkle free implant and to stabilize the shape of the implant and the breast over time. Soft gels (responsive) implants easily deform into a sphere by even a mild fibrous capsule while cohesive silicone gel implants retain their shape and form even when cut or compressed and hence breast shape remains stable ( Figure 6.1 ). A form stable, cohesive gel implant retains its shape even in unfavorable parenchymal environment such as thin soft tissues.
Advantages of form stable implants
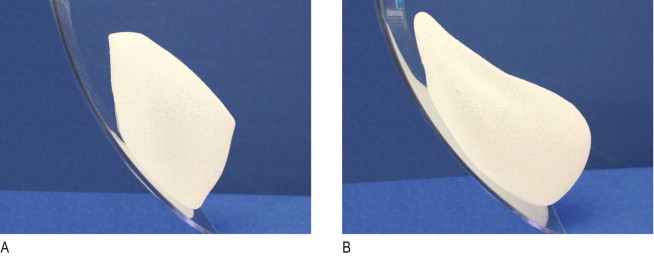
Form stable implants cause fewer deformities such as rippling, traction folds, buckling, knuckling, vertical implant displacement and bottoming out ( ). Our personal experience over the last decade has shown that the overall shape stays the same after a long period of implantation. Textured form stable implants move less during the capsular contracture compared with smooth, soft gel implants ( Figures 6.2, 6.3 ). The wide variety of different implant shapes and dimensions available today cater to more existing and desired breast types and makes customized fitting of an implant to a breast specific and individualized.

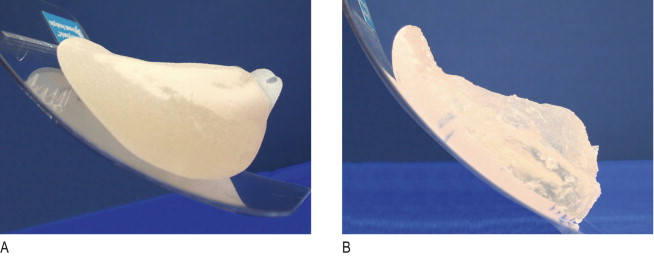
The high consistency of the filler gel influences the wear of the envelope. Improved device durability means less risk for implant rupture (0.3–1%). Hence, according to the same study, responsive gel implants have five to thirty times higher rupture risk and the removal of a ruptured, form stable implant is easy and more complete as the gel does not spread ( Figure 6.4 ). A well planned and executed, dimensional pocket with snugly fitting, elastic soft tissues overlying the stable shape implant better controls the final breast shape.
Disadvantages of form stable implants
Cohesive gel implants result in a slightly firmer breast, similar to Baker II consistency. While acceptable for young, nuliparous women, it may feel less favorable in multiparous woman with more softness, laxity and thinning of their breasts. Rarely, however, patients complained about firmness and in no instance were we asked to exchange form stable, cohesive gel implants to softer ones. The process of implant selection and surgical technique is more technically demanding with a need for a change in concept and a steeper learning curve for the surgeon. Because of the risk of damaging the implant by forcing it through a short incision, the incision must be larger (5.5–6 cm incisions are often necessary). In more than 90% of patients, the inframammary approach is the recommended route. Axillary and periareolar approaches are possible but less desirable. Using cohesive shaped implants carries 0.7% risk of rotation with major impact on the breast shape. The more complex technology of implant manufacturing has resulted in higher implant costs.
The gel confusion
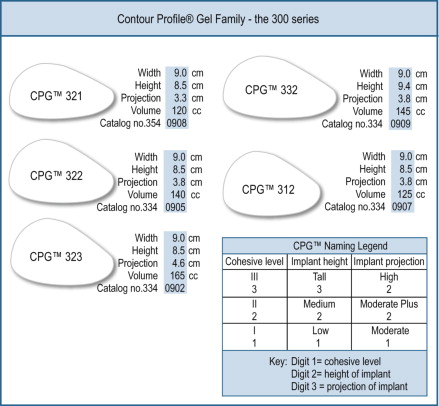
Since the introduction of the first high cohesive gel implant, it was obvious that cohesivity had no common denominator and that highly cohesive devices were different from each other in more than one way. Firmness depended on how much ‘cross linking glue’ was added to the original liquid formula. There is large variability related to the gel consistency amongst different manufacturers and in the way it is perceived by plastic surgeons. Consistency, degree of fill and shapes differ from one producer to another. Both major manufacturers, Allergan and Mentor, refer to their products as anatomical, high cohesive gel implants (Allergan: Matrix family, Style 410, 410 Soft Touch™ and Style 510 Dual Gel ( Figure 6.5 ). Mentor: CPG™ MemoryGel™ ( Figure 6.6 ). These two leading products differ not only in the fill but also in the feel and shape. It is impossible to compare both implant families in terms of gel consistency only by a subjective definition of examining and palpating the implants. The shape of anatomical and round implants produced by different companies is different. While it is clear that the final shape and the gel consistency are important for breast shape control, it is difficult to compare or verify which shape controls and creates a better looking breast in the same setting for a longer period of time.
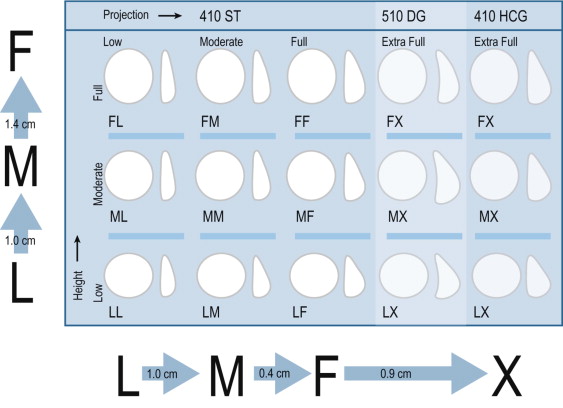
The Allergan (McGhan) Style 410 was the first shaped cohesive gel implant introduced. The expanded 410 product line includes 12 different shapes for any given width. Each implant is designated by width, and two letters. The first relates to the height (low, medium, full) and the second to the projection (low, medium, full). In 1997, the original high cohesive gel consistency was softened and the style 410 Soft Touch™ was added as an entire second matrix choice. An extra (X) projection implant was added 4 years ago forming a 12 ‘410 Matrix’. All original nine cells of the 410 series are available in the Soft Touch™ variety to cater to patients and surgeon’s needs and desires. It is not clear and there is no consensus whether softening the gel somewhat causes the implant to lose its shape primarily in the upper pole. There is agreement however that the thinner the soft tissue envelope of the patient, the more form stability is needed. In other words, a firmer shaped implant helps produces a better looking breast in thin patients.
The contour profile gel (CPG™) high cohesive gel from Mentor was initially made in a single shape (medium height, medium projection), and filled with a gel slightly softer than their competitors. In a series of Mentor’s gel consistencies from 1 (responsive gel), 2 (Lumera, similar to Soft Touch™), the new consistency was MemoryGel™ 3, the most highly cohesive gel in their series. The CPG line has later expanded to include three different projections and three additional heights. The huge choice of implant shapes and fillers further increases the ‘gel confusion’.
Patient selection
Both authors have had extensive experience using cohesive, form stable implants with a long-term follow up primarily with style 410/510 matrix family from Allergan. Ten years experience using cohesive, form stable implants in Europe and Israel clearly demonstrates the lowest reported incidence of rupture, fibrous capsule formation and reoperations rates ( ). Some misconceptions associated with breast augmentation need to be clarified, discussed, sharpened and nuanced before embarking on the journey of using form stable implants. Among them are that the only change caused by implants is size increase, that the implant does not cause changes in the breast tissues and that the implant’s fill, size or shape has no bearing on the long-term result. Implants firm up and lift the breast and therefore keep it looking young. Large implants permanently fill the upper pole and high profile implants correct breast ptosis. Round implants appear spherical and anatomical implants give a more natural but ptotic look.
Unsubstantiated working hypothesis like these are commonly verbalized by physicians and patients alike and require reeducation of both groups. Using the new cohesive, form stable implants requires a new way of thinking and a major paradigm shift from size to shape, from a fixed, steady state to a dynamic process, and from volume to dimensions. A recent large demographic study demonstrated that women are concerned about shape just about as or even more than about size ( ). Placing large implants under a limited and restricted soft tissue envelope weakens and displaces the fold and stretches the lower pole. This phenomenon ignores short- and long-term interaction between implant and soft tissues.
Thinning and atrophy of breast tissues due to heavy and extra-projecting implants make the final result unstable and less predictable. Soft tissue laxity and ptosis further complicates the task of breast enhancement and makes the process of implant selection even more crucial and more complex. The larger the implant, the greater the imbalance with the surrounding soft tissues and the less predictable the final result. Any implant may become a powerful manipulator of soft tissue and act as a tissue expander even if we do not want it to do so. Therefore if we want to shift from soft ‘responsive’ to cohesive ‘form stable’ implants, we need to change more than just our way of thinking.
Patient education, consultation, physical examination and measurements, implant selection, surgical technique and post-operative management must all be dealt with in a new and different way. Other questions that should be discussed prior to undertaking a major shift in clinical practice towards breast enhancement surgeries are concerned with the shape of the implant. Round or anatomical? Does implant shape influence breast shape? ( , ). Is there an identifiable characteristic shape for each device? Do round implants appear spherical while anatomical appear more natural? What are the indications and contraindications to use one or the other?
For practical purposes let us first consider young nuliparous patients presenting for primary breast augmentation with no ptosis, laxity or other signs of breast aging. Implant shape is chosen in such patients according to the thickness of the soft tissue coverage. Patients with a thick upper pole pinch could choose either a round or an anatomical device as the ample padding obscures the implant’s contours. On the other hand, patients with thin upper poles benefit more from an anatomical shaped device as round devices appear spherical even when placed underneath the muscle.
A well selected implant (dimension and size) that is in good equilibrium with the soft tissues of the patient will have a long-term rejuvenating effect on the breast whether it is round or anatomical, except that in our experience, shaped implants will better enhance the upper pole and therefore appear more natural ( ). In the parous patient or any patient with an aging breast (including young women with weight loss), a well selected shaped anatomical implant will better correct a mild ptosis when combined with controlled lowering of the inframamary fold and internal tissue manipulations as will be described below. This is true only for patients with a mild degree of ptosis and a reasonably good skin quality. Trying to correct second degree ptosis with a large, high-profile implant and lowering the inframammary fold is destined to fail.
No correction of patients with poor quality skin, skin excess, laxity and ptosis should be attempted using implants only. It is tempting at first to mistakenly assume that the new generation of form stable implants with the wide variety of shapes and profiles may obviate the need for tightening the envelope and lifting the breast. The wishful thinking that the lower pole curvature of a high profile, form stable implant may support and redrape the excess tissues in the inferior hemisphere of the breast and raise the nipple areola complex is not supported by our experience. The preferred approach remains mastopexy/augmentation using moderate size cohesive implants, avoiding future stretching, thinning, atrophy and recurrent ptosis.
While shaped (anatomical implants) seem to offer a better and more balanced upper pole fill with good projection under the nipple and areola complex, their use in patients with aging breasts and skin is fraught with a higher incidence of implant rotation. This tradeoff must be carefully discussed when selecting the shape of the implant. A recent study demonstrated an incidence of rotation of 0.7% over an 8-year period ( ). Implant rotation was typically more frequent during the early experience and was due to poor patient selection, improper surgical technique, primarily large pockets, seroma and early mobilization of the breasts.
To minimize rotation, there should be a perfect ‘hand in glove’ fit between the implant and the surrounding soft tissue envelope, no massaging, restricted upper torso exercising and gentle breast handling during sexual activity for 3 months. Patient education and consultation on form stable/high cohesive gel implants requires a different approach when compared with the traditional way of selecting a round, responsive gel implant ( ). The first step is usually conducted by a patient educator and contains information about shapes, gel consistency and available widths, heights and projections correlated with the patient’s desires and individual tissue characteristics. After viewing and feeling available consistencies and implants, patients are informed about the steps of selecting an appropriate implant. Often, a shaped implant is preferred to create shaped, natural and proportional results. Common and significant risks and complications are discussed, including the showing of photos of the most frequent complications to help create a realistic understanding of potential risks.
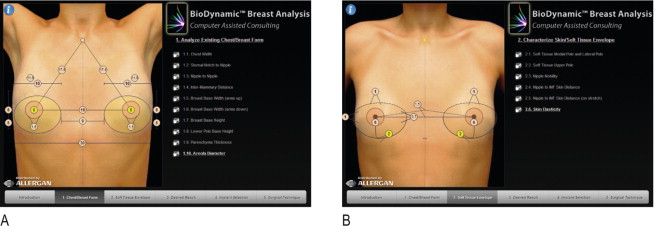
The second stage of the consultation process is done by the surgeon in front of a large mirror. The consultation process is more specific and directly oriented towards customized implant selection, related to and limited by the patient own tissues. Only through objective evaluation of the patient’s current breast and thorax can we dimensionally select the specific implant aimed to achieve the desired result. Dimensional patient evaluation considers current breast parenchyma, soft tissue envelope and the thorax. Some of the measurements (direct measurements) help in final implant selection while others (indirect measurements) are used to demonstrate and explain current asymmetries and limiting individual factors which may influence outcomes. Measurements and their interpretation with the patient’s active participation help create a realistic patient perspective about options, limitations, and outcomes.
To do this we are assisted with software (BioDynamic™ Breast Analysis System, distributed by Allergan) that guides the patient through a series of steps towards the final implant selection. First, we measure the patient’s thorax characteristics then the soft tissues ( Figure 6.7 ) Next, we enter into the software the patient desires regarding the size and shape of her future breasts ( Figure 6.8A ). This is followed by the actual implant selection where, within the limits of the patient’s characteristics, the software suggests the most appropriate available implant to fulfill her desires ( Figure 6.8B ). The final step simulates the prospective result using a family of external sizers suggested by the software. The sizers are placed inside a bra and an elastic T-shirt is placed over it ( Figure 6.9 ). Looking in a mirror, the patient provides her feedback to the physician. Based on this feedback, implant selection may be adjusted towards a smaller or larger implant (if possible).