Abstract
Secondary traumatic reconstruction of the temporomandibular joint (TMJ) remains a challenging prospect for treating clinicians when attempting to restore function and form of this complex joint which, in its native form, functions with both translational and rotational movements. Condylar fractures account for around a quarter of all mandibular fractures highlighting the common nature of this type of injury. Potential late complications of traumatic TMJ injuries include facial asymmetry, malocclusion, growth disturbance, osteoarthritis, and ankylosis with potential functional problems. Treatment modalities range from conservative to total joint replacement surgery, which largely depends on the extent of the problem and the clinical presentation. When the mandibular condyle is extensively damaged, degenerated or lost, replacement with either autogenous graft or alloplastic implant is an acceptable approach to achieve optimal functional and symptomatic improvement. The goals of TMJ reconstruction primarily are to improve mandibular form and function, to relieve pain where possible, provide cost-effective treatment, and to avoid complications and morbidity. Autologous TMJ reconstruction has included the use of the metatarsal graft, costochondral graft, coronoid process, scapula tip, iliac crest, sternoclavicular, deep circumflex iliac artery flap and of increasing recent use, the fibula free flap which is now widely accepted as the “gold-standard” for mandibular reconstruction. With now over 27 years of reported data, alloplastic devices have proven efficacy and safety, with outcomes similar or superior to standard orthopedic knee and hip prosthetic devices. Currently, TMJ Concepts (Ventura, CA) produces a patient-specific custom device utilizing CAD-CAM 3D technology, whereas Zimmer-Biomet Microfixation (Warsaw, IN) produces both stock (in the United States) and custom devices (not available in United States). Reconstruction of the TMJ is not without complications, the most common of all is postoperative infection, with other complications including heterotrophic bone formation and persisting pain.
Keywords
temporomandibular joint, TMJ ankylosis, secondary traumatic reconstruction, autologous, alloplastic, costochondral graft, fibula flap, stock device, custom device, TMJ prosthesis, Zimmer-Biomet, TMJ Concepts
Background
The temporomandibular joint (TMJ) is a complex and unique joint unlike any other joint in the body, with both translational and rotational function, and repetitive complex movement patterns to accommodate the functions of speech, mastication, and swallowing. For these reasons, posttraumatic secondary reconstruction of this joint remains a challenging prospect for treating clinicians, and as TMJ reconstruction is performed far less commonly than other joints (knee and hip), this limits clinical experience in the field but also limits the amount of quantitative data for qualitative analysis. Following traumatic injury, it is not only the bony components of the joint, namely the mandibular fossa and condyle, but also the ligamentous and fibrocartilaginous components that may sustain injury, particularly the articular disk and the fibrocartilage joint lining. Condylar fractures account for around a quarter of all mandibular fractures highlighting the common nature of this type of injury. Potential late complications of traumatic TMJ injuries include facial asymmetry, malocclusion, growth disturbance, osteoarthritis, and ankylosis with potential functional problems. There are a variety of treatment modalities to manage these problems ranging from conservative to total joint replacement surgery, which largely depends on the extent of the problem and the clinical presentation. When the mandibular condyle is extensively damaged, degenerated or lost, replacement with either autogenous graft or alloplastic implant is an acceptable approach to achieve optimal functional and symptomatic improvement. The goals of TMJ reconstruction primarily are to improve mandibular form and function, to relieve pain where possible, provide cost-effective treatment and to avoid complications and morbidity. Mercuri reported indications for alloplastic joint reconstruction that include ankylosis or reankylosis with severe anatomical abnormalities and failed autogenous grafts in multiply operated patients. In this chapter, we will discuss these indications further, with emphasis towards posttraumatic secondary reconstruction.
Autologous TMJ reconstruction has been described in the literature since the early 1900s and has included the use of the metatarsal graft, costochondral graft, coronoid process, scapular tip, iliac crest, sternoclavicular, deep circumflex iliac artery flap and of increasing recent use, the fibula free flap. Indeed, with improved understanding and technical abilities of the reconstructive surgeon, autologous microvascular reconstructive techniques are now widely accepted as the “gold standard” for mandibular reconstruction. In the 1970s and 1980s, alloplastic joint reconstruction resulted in significant complications associated with prostheses containing Proplast–Teflon, where fragmentation on prolonged cyclical loading often resulted in a very locally destructive foreign body giant cell reaction. The subsequent litigation and FDA recall of these devices in the United States placed progress on hold for a period until the early 1990s where newer improved devices were introduced to the market. Currently, TMJ Concepts (Ventura, CA, USA) produces a patient-specific custom device utilizing CAD-CAM 3D technology, whereas Zimmer-Biomet Microfixation (Warsaw, IN, USA) produces both stock (in the United States) and custom devices (not available in United States). With now over 27 years of reported data, these devices have proven efficacy and safety, with outcomes similar or superior to standard orthopedic knee and hip prosthetic devices. Some common autologous and alloplastic TMJ reconstructive modalities will be discussed further in this chapter.
Anatomy of the TMJ
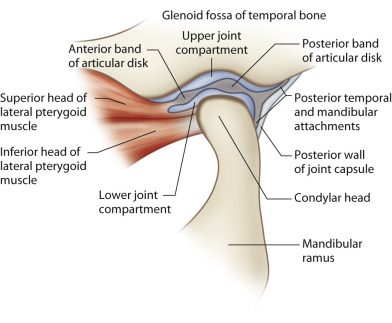
The TMJ is a bilateral ginglymoarthrodial (hinging and sliding) synovial joint between the condylar head of the mandible and glenoid or mandibular fossa on the undersurface of the squamous part of the temporal bone, together making a craniomandibular articulation (see Fig. 3.10.1 ). The joint is separated into an upper and lower compartment by a fibrocartilaginous disk that is biconcave in shape against the articulating surfaces within both compartments. The bony joint surfaces are covered with the same fibrocartilage which is less susceptible to degeneration and has a greater repair ability compared to hyaline cartilage found in other synovial joints. The mandible from condyle to condyle is a continuous entity and therefore movement in either TMJ is dependent upon the other whilst the extent and direction of movement is determined by the articulating surfaces, ligaments, and local musculature.
The collateral, capsular, and temporomandibular ligaments are direct anatomic components of the TMJs whilst the sphenomandibular and stylomandibular ligaments are attached at a distance from the joints. Collectively, they provide stability and control joint movement.
The muscles of mastication are the masseter, temporalis, medial pterygoid, and lateral pterygoid. The accessory muscles of mastication include the suprahyoid (digastric, geniohyoid, mylohyoid, and stylohyoid), and infrahyoid (sternohyoid, omohyoid, sternothyroid, thyrohyoid) muscle groups. When the mouth is opened, the condylar head undergoes rotation in the lower joint compartment while an anterior gliding motion occurs in the upper compartment. The lateral pterygoid and digastric are the main muscles involved in mouth opening whilst the masseter, temporalis, and medial pterygoids are the key muscles involved in mandibular elevation and subsequent mouth closure.
Posttraumatic Indications for TMJ Reconstruction
The potential long-term sequelae of TMJ trauma that may require reconstruction and management are:
- •
Ankylosis
- •
Condylar malunion/malposition with malocclusion and/or facial asymmetry
- •
Degenerative joint disease
- •
Failed primary reconstruction (autogenous/alloplastic)
Ankylosis
Posttraumatic ankylosis of the TMJ injury is an uncommon complication of condylar injury and is of particular concern in pediatric cases where significant growth disturbances may result. This includes facial asymmetry, retrognathism, and secondary midface growth deficiency. In the adult patient, it may present as trismus with resultant compromised mastication, speech, oral hygiene, and even psychosocial distress. This complication usually results from comminuted intracapsular injuries, particularly when the articular disk is disrupted. It has also been suggested that concomitant anterior mandibular fractures, which allow posterior facial widening and consequent lateral displacement of fractured condyles, also increase the risk for this complication. Treatment can depend on the severity of the condition with various treatment modalities at the clinician’s disposal, including gap arthroplasty, costochondral grafting, and total joint replacement. The growing patient offers additional reconstructive challenges and often requires further corrective surgeries consequential of dynamic changes in the growing patient. Complete bony TMJ ankylosis has been typically managed with gap arthroplasty, autogenous tissue graft or alloplastic arthroplasty. Autogenous grafting techniques usually require a period of immobilization postoperatively to allow adequate healing and limit the risk of graft failure resulting in mandibular functional delay. The lack of early mobilization and lack of soft tissue interface can risk reankylosis and should this occur, then total alloplastic reconstruction may be considered. In the growing patient, ankylosis of the TMJ may lead to asymmetrical mandibular growth resulting in height reduction of the affected ramus and subsequent facial asymmetry with chin deviation to the affected side, due to normal growth of the opposite side and impaired growth of the affected side. Compensatory occlusal disturbances may also occur such as overeruption and tipping of teeth to help reestablish functional occlusion. TMJ ankylosis in growing subjects has traditionally been managed by autogenous grafting, with the costochondral grafts as the most widely used method for these TMJ reconstructions. The rationale for autologous grafting is to maintain growth potential but growth and resorption can be unpredictable and other complications such as ankylosis have been reported.
Sawhney classified four types of pathological changes in the ankylosed TMJ. Type 1 describes flattening of the condylar head with surrounding dense fibrous adhesions making movement impossible. Type 2 includes a flattened or deformed condylar head, with close proximity to the articular surfaces, and a limited bony fusion of the outer, anterior or posterior surface. Type 3 includes a bony block bridging across the ramus and the zygomatic arch, with the displaced articular head fused to the medial side of the ramus, or the presence of an atrophic condylar head. Type 4 presents as a large bony block that completely replaces the usual joint architecture.
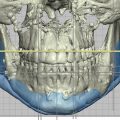
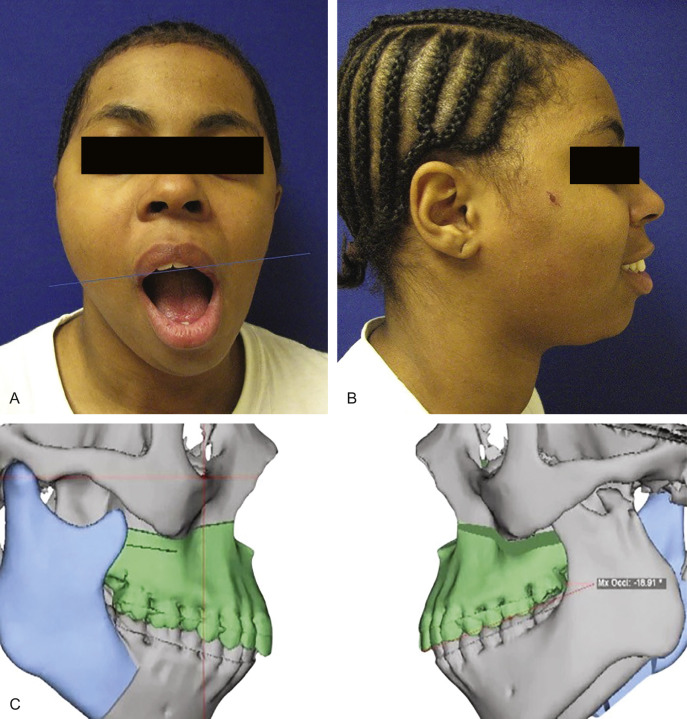
Condylar Malunion/Malposition With Malocclusion and/or Facial Asymmetry
Loss of posterior mandibular vertical dimension due to traumatic injury can cause occlusal discrepancies as either an anterior open-bite where bilateral mandibular height is lost, or premature contact of the posterior teeth with contralateral open-bite where there is unilateral vertical height loss. Fig. 3.10.2 illustrates left condylar hypoplasia and the resultant loss of left vertical height in a young patient following an old traumatic fracture dislocation injury. In the absence of successful primary trauma reconstructive surgery or other management to help reestablish normal vertical height and correct occlusal discrepancies, then joint reconstruction (autogenous or alloplastic) or osteotomy may be considered. In the growing patient, loss of vertical height on the affected side may either be due to ankylosis and the resultant hypomobility or from direct injury to the condylar cartilaginous cap. It has been widely accepted for the growing patient where preservation of growth potential is desired, autogenous grafting such as the costochondral graft, is preferred over alloplastic TMJ reconstructive solutions. However, very good results using alloplastic devices in growing patients are emerging, with maintenance of facial symmetry in both unilateral and bilateral cases.
Degenerative Joint Disease
Traumatic injury to the TMJ, whether direct or indirect, can lead to osteoarthritic changes within the joint. Posttrauma joint effusion is well known in the orthopedic literature and has frequently been observed in posttraumatic imaging of the TMJ by magnetic resonance imaging (MRI), whilst other studies have shown arthroscopic evidence of TMJ articular damage following mandibular fracture injuries. The proinflammatory cytokine interleukin-6 (IL-6) has been shown to play a key role in the pathogenesis of arthritis and has been found in higher concentrations in TMJs with internal derangement and osteoarthritis when compared to TMJs without joint effusion. Nogami et al. found a correlation between MR evidence of joint effusion and concentration of IL-6 in washed-out synovial fluid samples collected from patients with mandibular condyle fractures. TMJ arthritis is one of the most common diseases affecting this joint and has a variety of other etiologies besides trauma, including inflammatory, infectious, metabolic, degenerative osteoarthritis, and systemic arthritides. Therefore, where preexisting disease is present, then certainly a traumatic insult can exacerbate the primary disease state. Symptoms depend on disease progression but patients may typically present with constant preauricular pain, with or without radiation and crepitus. Other symptoms may include TMJ locking, clicking, popping, and mandibular deviation on opening. Although a majority of patients earlier in the disease process will respond to nonsurgical treatment modalities or limited surgical intervention, when the mandibular condyle is extensively damaged, degenerated or lost, replacement with either autogenous graft or alloplastic implant is an acceptable approach to achieve optimal functional and symptomatic improvement.
Autogenous Graft Failure
The success of nonvascularized autogenous tissue reconstruction in part depends on the quality of the vascular bed at the host site, which is often compromised due to the presence of dense fibrous tissue from the trauma and also prior surgery. Marx reports that scar tissue surrounding previously operated bone averages 440 µm in thickness, however capillaries can penetrate a maximum thickness of 180–220 µm of tissue, which would significantly compromise graft viability and in certain cases may explain autogenous graft failure. Auricular cartilage was once widely advocated for autogenous disk replacement, however subsequent studies have suggested it is not an ideal substitute and patients treated this way primarily for posttraumatic disk replacement with subsequent graft failure, may require secondary reconstructive surgery. Patients reconstructed with autogenous costochondral grafting normally undergo 4–6 weeks of maxillomandibular fixation following which the mandible is returned to functional activity to prevent ankylosis. However, Reitzik reported that cortex-to-cortex healing of the vertical ramus probably requires 25 weeks in humans following studies on monkeys. Micro-motion of these free grafts will invariably occur with early mandibular functional movement resulting in compromised graft success. Furthermore, both vascularized and nonvascularized reconstructions may fail due to ankylosis, especially if there is no soft tissue interface between the condylar reconstruction and glenoid fossa of the temporal bone.
Alloplastic Joint Reconstruction Failure
Many patients who underwent TMJ reconstruction in the 1970s and 1980s with Proplast–Teflon coated alloplastic prostheses or Silastic developed foreign body giant cell reactions with subsequent osteolytic changes around the devices. The resultant bony destruction and often multiply operated surgical sites rendered the locally distorted anatomy challenging to manage. Henry and Wolford reported less success with autogenous bone and soft tissue grafts in patients who had previously had Proplast–Teflon or Silastic in place. Henry and Wolford also reported in the same study that reconstruction with autogenous materials was much less predictable than with alloplastic replacement. It is therefore reasonable to consider total alloplastic TMJ reconstruction in this group of patients to achieve optimal postoperative functional value.
Imaging of the TMJ
TMJ imaging of the appropriate nature and quality is fundamental for diagnostic evaluation and treatment planning in the TMJ patient. Although conventional imaging (such as panoramic radiography) is cost-effective and with lower radiation exposure compared to more advanced imaging modalities, it only provides two-dimensional detail. With superimposed regional anatomy over the region of interest, it is often necessary to take films in different planes to accomplish the detail required for diagnostic and planning purposes. For this reason, coupled with the potential for artefacts and other processing errors, conventional radiology is not the primary choice for TMJ imaging when considering secondary TMJ reconstruction where greater imaging accuracy and detail is required. However, conventional imaging or plain film still remains a useful initial study.
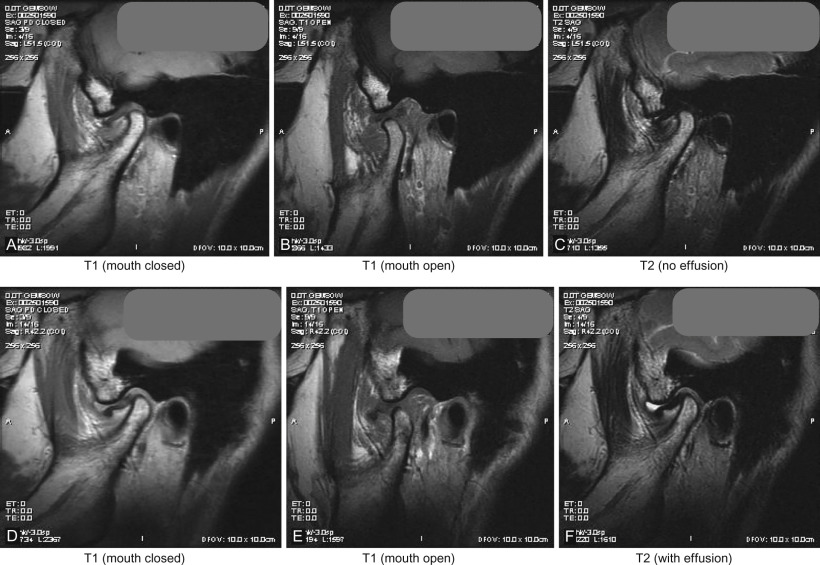
Computed tomography (CT ) permits detailed assessment of the TMJ, allowing views in the axial, coronal, and sagittal planes and also makes 3D volumetric reconstruction possible. CT is particularly useful in the assessment of bony structures and pathologies such as TMJ ankylosis. Indeed a “bony window” setting helps accentuate this effect, while a “soft-tissue” setting helps visualize nonosseous structures more clearly. However, despite the latter, the TMJ disk and other soft tissue structures in the region of interest are often impossible to view with CT alone. Higher radiation exposure and cost can be brought down considerably with the use of cone beam computed tomography (CBCT) technology but image artefacts from metallic objects, whether dental restorations or metallic prostheses near or in the field of interest, produce a starburst pattern of scatter. This may mask the detail required for TMJ assessment and other image modalities may be sought. Magnetic resonance imaging (MRI) is widely accepted as the study of choice to visualize the TMJ disk and ligaments, adjacent soft tissues, inflammatory changes, and the presence of joint effusion. Depending on image weighting, two commonly used studies are T1 images, which are fat-enhancing and provide excellent anatomic detail such as disk position/displacement, and T2 imaging, which is used in identifying inflammatory processes and/or the presence of joint effusion in the TMJ. Open and closed views (see Fig. 3.10.3 ) are captured to understand changes in joint biomechanics and disk pathology. As with CT imaging, artefacts can occur with metallic objects such as dental restorations. Aneurysmal brain clips or patients with indwelling cardiac pacemakers are contraindications for MRI study. Volumetric 3D reconstruction is also not easily achievable unlike with CT imaging, however Costa et al. conducted a study to define the diagnostic value of a method for 3D reconstruction of MRI images for the assessment of TMJ and found the method to be a useful and an accurate tool for this purpose, particularly when focusing on internal derangement.
TMJ Reconstructive Techniques
Autogenous TMJ Reconstruction
In 1909 Bardenheuer first replaced the mandibular condyle with a patient’s fourth metatarsal and in 1920 Gillies introduced costochondral grafts (CCGs) for condylar reconstruction. Autogenous grafting techniques have since continued to develop and have been of particular significance in the growing patient where preservation of growth potential has remained of primary importance. Although other grafts, for instance coronoid process, scapular tip, fibula, sternoclavicular joint and iliac crest have all been employed in TMJ reconstruction, the most widely used has been the costochondral graft, particularly in the child patient.
Costochondral Graft
In 2000, McIntosh reported advantages including biological compatibility, workability, functional adaptability, minimal donor site morbidity. Kaban et al. published a protocol employing CCGs for the management of TMJ ankylosis in children demonstrating excellent growth potential. However, disadvantages of costochondral grafting include donor site morbidity, fracture, ankylosis, and unpredictable growth. Kaban suggested the most frequent source of failure in children treated for TMJ ankylosis has not been a lack of patient cooperation but, rather, inadequate ankylosis release. This is most commonly caused by a failure to adequately excise the ankylotic mass, resulting in failure to achieve complete, passive opening (without the need for excessive force) in the operating room. In 1999 Ko et al. reported a study involving 10 children all of whom underwent CCG reconstruction to manage TMJ ankylosis with a mean age of 7.4 years, two of whom had bilateral TMJ ankylosis. Ko further reported progressive deviation of the chin toward the nonaffected side in five of the children after TMJ reconstruction. The study found CCGs tended to have a more vertically directed condylar growth pattern and a more laterally positioned condyle, in the two cases with bilateral TMJ reconstruction, the CCGs grafted grew until there was a mandibular prognathism that required corrective surgery. To minimize the risk of overgrowth, it has been suggested to limit the thickness of the cartilaginous cap. In 2003, Saeed and Kent conducted a retrospective review of 76 CCGs (57 patients) to determine outcome with respect to the extent of previous surgery (none, disc surgery or soft tissue graft, alloplastic disc, alloplastic joint, previous graft) and to initial and preoperative diagnosis. They concluded in patients with no previous surgery, arthritic disease or congenital deformity the costochondral graft performed well but in patients with previous alloplastic discs and/or total joints the results were less predictable. A preoperative diagnosis of ankylosis was associated with a high complication and further surgery rate suggesting caution in this group of patients. CCGs can be used as an initial TMJ reconstructive approach for the adult post-traumatic patient but resorption can be problematic and for this reason, nowadays CCGs are less frequently used when compared to other autogenous options such as the fibula flap. Medra reported 85 cases of CCGs for TMJ reconstruction and follow-up demonstrated resorption in 21 patients (25%), of which 10 patients showed partial resorption and 11 had complete resorption of the grafted bone.
Vascularized Fibula Free Flap
The fibula free flap (FFF) has become a widely accepted autologous reconstructive option for segmental mandibular defects after resections for cancer, benign tumors, trauma, or osteonecrosis. Advantages of this flap include the ability to repair soft-tissue composite defects, excellent bone length that can be shaped to fit the anatomical need, vascularized bone that resists resorption, suitability for dental implant placement and so allowing dental rehabilitation, and finally the ability to have a two-team approach reducing anesthesia time. Garcia et al. reported six patients who underwent mandibular resection including the condyle and reconstruction using FFF where in all the cases, the fibula was placed directly into the glenoid fossa. The temporomandibular disc was preserved over the condylar end of the fibula. Panoramic radiographs were performed postoperatively to evaluate condylar position and grade of bone resorption. Five of the patients developed good function whilst one fibula ankylosed, concluding the use of the FFF directly fitted into the glenoid fossa is a reliable method in condylar reconstruction but the risk of ankylosis persists. Other options include fitting a prosthetic condyle onto the fibula to articulate against the articular eminence or where the native condyle is preserved, then this can be fixated directly onto the fibula graft. Figs. 3.10.4–3.10.8 illustrate secondary reconstruction of the TMJ with a fibula graft where primary reconstruction failed after many years.