21 Secondary rhinoplasty
Synopsis






Introduction
Why secondaries are difficult
If rhinoplasty is the most difficult operation in aesthetic rhinoplasty then surely secondary rhinoplasty is even more difficult.1 The overall revision rate of 20% suggests that this is the case. Whereas, the patient who needs a revision rhinoplasty is willing to let the first surgeon perform it, he/she is much less likely to allow a third procedure by that surgeon if, for whatever reason, there is dissatisfaction once again. It behooves the surgeon therefore in a revision rhinoplasty to do everything possible to avoid an unhappy patient with its concomitant problems (law suit and public complaining on the internet).2
Patient selection
Nasal evaluation
JP Gunter3 has probably done more than any other surgeon to emphasize the importance of analysis. Kim and Toriumi4 have a complete review on this subject and Pessa and Rohrich cover this subject in Chapter 17. We would like to emphasize what we consider the most important aspect of analysis in our practices: the use of digital imaging.
It behooves the surgeon to use imagers (Fig. 21.1) for preoperative planning for each patient. Imagers are widely available and economical. It is helpful to demonstrate to the patient what you think should to be done and eliciting their feedback as to what they think should be done. The patient needs to know what can and cannot be realistically achieved. In the process of imaging, the surgeon him/herself learns what problems may exist. Sometimes, the process of morphing can be enlightening. Often what may appear to be the problem when judging the patient sitting in the examining chair is not the problem as seen by the camera on the monitor. Conversely, some anatomic problems only become obvious when on the monitor. Patients with unrealistic expectations can be weeded out by this process. Above all, morphing with an imager is a form of mock surgery.

Operative techniques
Artistry in rhinoplasty
It is not enough to have the knowledge of nasal anatomy.5 Rhinoplasty is sculpting with a biological medium (cartilage and some bone). As such, we need to employ an artist’s principle: copying. It is much easier to copy a beautiful structure than it is to create it from memory. Commercial artists rely on this concept. Unless you are a naturally gifted artist, you will find this to be the case. Few of us can draw a decent picture of a cat from memory, but even an artistically challenged individual can copy a reasonable facsimile of a cat from a photograph. Consequently, we recommend the use of an intraoperative model of the ideal or prototype nasal framework (Fig. 21.2). It saves the effort of memorizing facts (e.g., how much the tip should be elevated above the dorsum; what the width of the lateral crus should be; what the angle of divergence is, etc.). Magnifiers and loupes make it difficult to see the nose from a distance and get the proper perspective. Therefore, it is also helpful to have a video camera in the operating room (which gives a profile view of the patient (from a distance) at all times). It is not surprising that some surgeons are on occasion perplexed to see that the patient’s nose has nostril exposure the next day or at the time of splint removal. They may have neglected to judge that angle accurately when the patient was in the supine position. Stepping back to evaluate the patient, or using a video camera, gives a better perspective and helps avoid this problem.





The open versus closed approach in secondary rhinoplasty
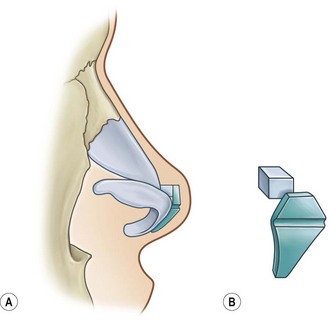
The decision to open the nose or not in a secondary can be more difficult than in the case for a primary rhinoplasty.6 If there is little to do, e.g., rasping the dorsum or attaching a rim graft, there is no question that a closed approach is ideal. And if it appears that visualization will be beneficial to completing the task, e.g., straightening the nose, or straightening out a twisted tip, there will be little questioning that an open approach will permit greater accuracy and therefore a better final result. However, there are many less clear cut cases. For example, if the patient has had multiple prior surgeries with a thick round fibrous tissue filled ill-defined tip the decision is much more difficult. That is because opening the nose (whether there is an existing columellar scar or not) has the potential for even more edema and subsequent fibrosis to the tip. In the nose with thick skin, fibrous tissue deep to that skin can be a surgeon’s nightmare (Fig. 21.3). Further surgery, no matter how precise in terms of achieving a finely sculpted framework, can aggravate the thickness problem and give a worse result. The best approach in these kinds of cases is to select a surgical plan that minimizes surgical trauma and undermining. It is best to consider an open approach in this case, only if it is felt necessary that some surgical maneuvers will be impossible to achieve without it, e.g., lengthening the nose.


Anesthesia
Most of our patients receive conscious intravenous sedation because it is less costly to the patient. The overall benefits of conscious sedation are reviewed elsewhere.7 Unfortunately, many residency programs do not train surgeons to use it, forcing them to learn it following their formal training. Patients are instructed to take Flurazepam (Dalmane) 60 mg 1 h prior to arriving at the surgery center. On arrival, the relaxed patient then receives IM Hydroxyzine (Vistaril), 100 mg and IM Nalbuphine (Nubain) 10 mg. Demerol 50 mg can be used as an alternative to Nalbuphine. In the operating room, the patient is sedated with incremental 1 mg doses of Midazolam (Versed). When the patient has difficulty counting backwards from 100, Ketamine 30 mg is given slowly over 30 s. For larger female patients and males, 50 mg is employed. Additional incremental doses of Versed (1 mg) are used if the patient should not enter that desired “dissociative state” that Ketamine is known to produce, which lasts for approximately 5 min.
Suture techniques versus grafts
Suture techniques
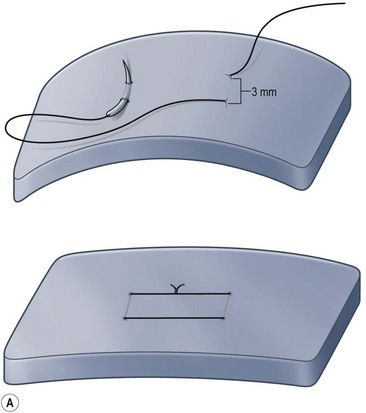
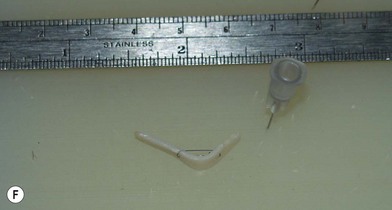
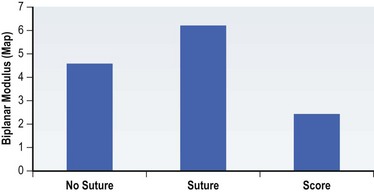
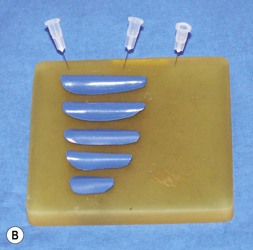
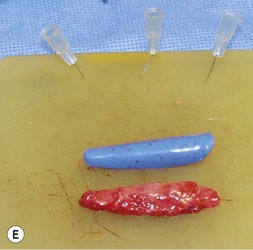
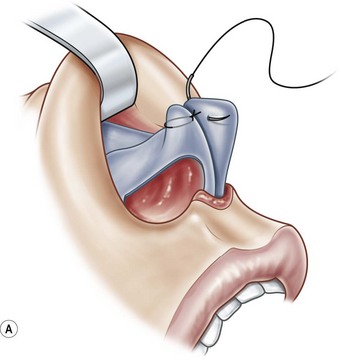
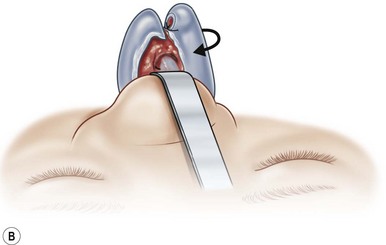
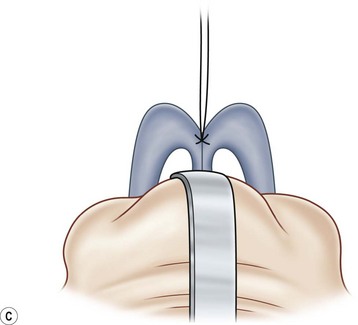
The universal horizontal mattress suture8,9 is a suture that can be applied to any unwanted convex or concave cartilaginous structure of the nose in a secondary rhinoplasty. A short learning curve is necessary because if the gap between purchases is too little, no effect results but if the gap between purchases is too large, the cartilage will buckle (Fig. 21.4). Our studies have shown that one suture can increase the strength (biplanar modulus in engineering terms) of the cartilage by approximately 35%, whereas scoring the cartilage to achieve the same degree of correction can weaken the cartilage by as much as 50% (Fig. 21.5). The lateral crural mattress suture is the most obvious example. However, the universal horizontal mattress suture is also useful for wanted curvatures of the septal L-shaped struts. Ear cartilage is much more usable when it is straightened and stiffened with this particular suture. When the concha cymba is removed from behind the ear, it is split down the middle, pinned to a silicone block, concave side down. A 5-0 PDS horizontal mattress suture is applied at each end of the cymba to straighten it and stiffen it (Fig. 21.6). Such a suture reinforced graft makes a good columellar strut and can even replace the entire lateral crus if it is missing.









Grafts
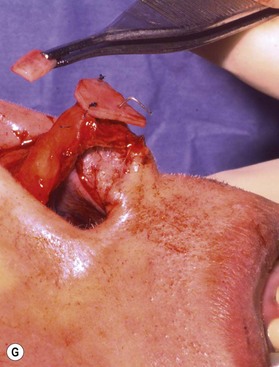
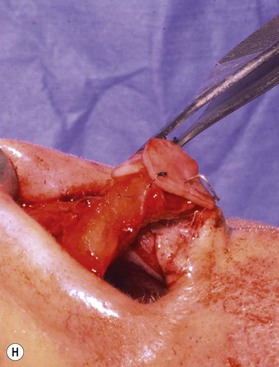
Most secondary rhinoplasties demand grafts to either replace missing cartilage that has been excessively removed or to provide support for weak structures. Septal cartilage is preferred. However, it is usually unavailable in sufficient quantities. Therefore either ear or rib is required. For small amounts of cartilage, we prefer ear cartilage. Since it can be straightened and stiffened as described above, it is useful for almost ever situation where septal cartilage would ordinarily be used. However, when large amounts of cartilage are required, we prefer rib.10,11 In particular we prefer the 5th rib that is accessible from an inframammary incision (Fig. 21.7). The entire rib need not be removed. The anterior half is relatively easily removed with a slightly curved 1 cm osteotome and/or a septal knife.


If structural support is not needed, cartilage grafts need not be solid in order to reconstruct noses. Diced cartilage has a vital role, especially if it is wrapped in a substance like fascia to give it shape. This technique was developed primarily for dorsal augmentation by Daniel.12 Erol13 demonstrated that diced cartilage in a Surgicel wrapping could be useful. However, the authors prefer fascia to avoid the possibility of absorption due to the slight toxic effect of Surgicel. The cartilage is cut into small bits approximately 1 mm in size and placed in a blanket of fascia (on a silicone block). The fascia is simply folded over and secured with 5-0 plain catgut suture. It is helpful to have applied a silicone sizer in the patient’s dorsum, to get an idea as to how long and thick to make the diced cartilage graft (DCF) graft (Fig. 21.8).



One option we do consider for reconstruction in secondary cases is the use of irradiated allograft rib cartilage. This can be useful when the patient is resistant to harvesting autogenous material. The main problem with allograft, of course, is the potential for absorption. Although some reports of long-term survival exist,14 one must be prepared for absorption approximately 10 years postoperatively. An option we never consider for secondary rhinoplasty is the use of implants of any material. We recognize that many surgeons have found them helpful because they are easy to employ and economical for the patient. However, occasional failures (risk of skin necrosis and implant exposure) although unlikely, can be exceedingly difficult to correct when they happen.
Common problems
Broad, bulbous, round tip
General approach
One of the most common frustrations in secondary rhinoplasty is the broad, or bulbous or round tip.15 Patients complain about this most often and most vigorously. Fortunately, there are some good solutions. It is important to decide whether to use the open or closed approach for the reasons mentioned above. Most of the time, the cephalic part of the lateral crus has been resected at the first surgery. In fact, too much has often been removed. The first goal is getting to the abnormal tip anatomy. In the open approach, careful elevation of the flap is necessary. In the closed approach, it may be necessary to deliver the tip cartilages with an intercartilaginous and marginal incision. The second goal is to establish a lateral crus that is approximately 5–6 mm wide and render it straight. Usually, suture techniques will convert the existing tip framework into something that is more normal and stronger.
Tip-plasty by suture techniques (Fig. 21.9)






Suture techniques are one of the main means by which the framework is modified.15–20 The many types of suture techniques that apply to the primary rhinoplasty apply equally to the secondary rhinoplasty, although fewer are necessary because some of them have usually been applied at the first surgery. Guyuron and Behman et al.15,16 have reviewed most of the common techniques. Daniel17 has a useful algorithm and we have one that deals with most problems. Our own suture algorithm for tip-plasty involves four basic sutures: (1) hemi-transdomal; (2) lateral crural mattress suture; (3) interdomal suture; and (4) columella-septal suture. The hemi-transdomal suture21 is a variation of the transdomal suture that narrows the dome. It is placed at the cephalic end of the dome so that it everts the caudal rim and prevents rim collapse or concave rims. The hemi-transdomal suture minimizes the need to use rim grafts which are often used to maintain a straight nostril rim or prevent concave rims. Daniel17 and Toriumi22 were aware of the importance of having a suture at the cephalic end of the dome. The lateral crural mattress suture removes any residual convexity of the lateral crus. One, two or even three such sutures will flatten out the lateral crus and make it strong. This is especially useful in secondary cases because the lateral crurae are often weak from the first surgery with residual convexity. The interdomal suture brings the domes together and provides a small amount of tip rigidity and symmetry. The columella septal suture secures the tip to the caudal septum. One can adjust the height to some degree with this suture, although it is not a substitute for the columellar strut. All of these suture techniques require either 5-0 nylon or PDS. If one is certain there is good soft tissue coverage, a permanent suture such as nylon is a reasonable choice. Figure 21.9 is an example of a patient who had multiple prior surgeries and grafts. She required sculpting of the tip cartilages with suture techniques. In addition to the four suture algorithms described above, she required a humpectomy and osteotomies.
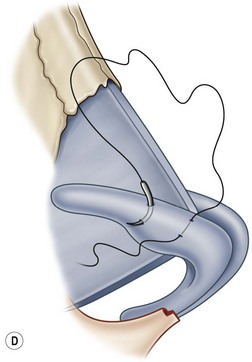
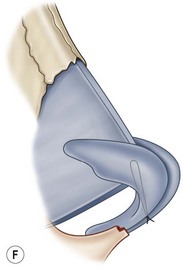
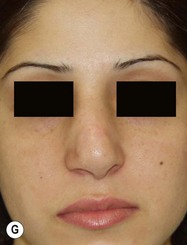
Closed approach
Some secondary noses simply do not warrant the extensive dissection associated with closed method of tip delivery or the open approach. Some patients are unhappy with their existing scar and are nervous about another open approach. These cases are benefitted by cephalic resection of the lateral crus alone. This is done by way of an intracartilaginous incision. All the cartilage (of the lateral crus) cephalic to the incision is removed. The decision is guided by what the minimal surgery is necessary to achieve the goal. Figure 21.10 is a good example of a broad tip problem (Fig. 21.10). The patient exhibited a broad tip, supratip deformity, and radix deficiency. Because of the very thick skin and her nervousness about the scar, it was decided to use a closed approach. The tip cartilages were delivered. The patient received cephalic trim of the lateral crus along with interdomal and lateral crural mattress sutures (5-0 PDS). A radix graft was used and the caudal septum was shortened. A lateral osteotomy was also performed.