Abstract
Traumatic injury to the bony midface and mandible is typically accompanied by consequent disruption of normal occlusion. While this is optimally managed in the primary setting, all too often fractures are inadequately reduced, resulting in a healed malocclusion. Once this has occurred, the only option for correction is a secondary surgery that is much more complicated due to scarring and the necessary surgical maneuvers involved. Upon presentation, patients must be thoroughly evaluated through physical examination and imaging with computed tomography (CT) in order to obtain a complete picture of the pathological anatomy. Careful planning of osteotomies of the involved bony structures should be undertaken, either with virtual surgical planning or traditional model surgery techniques, and making use of intraoperative occlusal splints, such that premorbid occlusion is restored.
Keywords
secondary osteotomies, maxilla, mandible, occlusion management
Keywords
secondary osteotomies, maxilla, mandible, occlusion management
Background
Unless there has been a loss of substance of portions of the maxilla and mandible, most traumatic disruptions of the maxilla and mandible are well corrected by placing the patient in the pretraumatic dental occlusion, plating the fractured segments with titanium miniplates and screws, and maintaining intermaxillary fixation where required. In extensive maxillary fractures, autogenous bone grafting is performed to reestablish the buttresses correcting the maxillary alveolus to the base of the skull. It is rarely indicated to do primary bone grafting of the mandible. This of course presumes that the surgeon treating the jaw fractures, whether an oral surgeon or plastic surgeon, has an adequate knowledge of dental occlusion and the availability of a dental lab to fabricate splints when needed. If treated adequately, fractures of the tooth-bearing segments rarely require secondary surgery.
However, when there are concomitant fractures of the facial skeleton involving the upper segments of the midface – the orbital cavities and zygomatic arches – it is not rare at all to see significant deformities requiring osteotomy and repositioning of malpositioned segments. Joe Gruss has said that one of his fellows coined the wonderful acronym “OIF” for these situations – where the surgeon did open rigid fixation of the fracture, without the “R” of reduction. The reason for this is reluctance by the inexperienced surgeon to adequately expose the fracture sites through a coronal incision, and a hesitation to use autogenous bone grafts for the internal orbit and nose. This hesitation finds a comfortable option to avoid autogenous bone with the availability of a variety of alloplastic materials, so-called “bone substitutes,” such as methylmethacrylate, titanium mesh, silicone, MedPore, hydroxyapatite, etc. It is best to eschew the use of all of these materials – there is simply no better bone substitute available than fresh autogenous bone grafts. If there is a reluctance and hesitation to use them, then the solution is better training of surgeons in safely harvesting and using autogenous bone grafts so that they are comfortable in doing so.
Sir Harold Gillies, writing in 1920, put it eloquently: “There is no royal road to the fashioning of the facial scaffold by artificial means: the surgeon must tread the hard and narrow way of pure surgery. Of the various autologous grafts available one has had enough experience to form some conclusions. It may be laid down as the guiding maxim that the replacement should be as nearly as possible in terms of the tissues lost, i.e., bone for bone, cartilage for cartilage, fat for fat, etc.” In the cases that will be shown here, this advice has been followed.
Patient Evaluation
Physical Examination
Upon initial presentation, a focused physical examination will identify most of the issues that will need to be addressed. Regarding bony structural deformities of the mid-face, bony step-offs and obvious facial asymmetries may be apparent if there are inadequately reduced fractures. Vertical orbital dystopia, enophthalmos, or telecanthus are findings indicative of orbital floor, zygomaticofacial, or naso-orbital-ethmoidal (NOE) fractures that will require correction.
While occlusion is frequently described using the Angle classification, this is often less important in the setting of midface trauma with occlusal deformities. Patients will often not have optimal dentition, and it is usually more beneficial to focus on determination of the patient’s premorbid occlusion using the “fit” of the maxillary and mandibular teeth based on complimentary wear facets with the mandibular condyles seated in the fossa of the temporomandibular joint. There are additional findings that are relevant in diagnosing and describing occlusal deformities, and can assist in developing a surgical plan – specifically, the presence of an occlusal cant, mandibular deviation on opening, presence of an anterior open-bite, or a lateral crossbite. The presence of an obvious cant can suggest a laterally impacted or otherwise malpositioned maxillary segment, and/or nonreduced unilateral mandibular condyle fracture. Dynamic mandibular deviation or a lateral crossbite are also typically suggestive of untreated unilateral condylar pathology, while an anterior open-bite is likely due to inadequately reduced bilateral condyle fractures. Obvious step-offs in the anterior mandibular occlusion are frequently related to untreated parasymphyseal fractures.
Imaging
A maxillofacial computed tomography (CT) scan with thin cuts and 3D reconstruction is of the utmost importance to properly evaluate fractures of the craniofacial skeleton, both acutely and secondarily, and should be obtained in all cases of facial trauma. The axial, sagittal, and coronal views permit the surgeon to accurately assess bony deformities in multiple planes, and take accurate measurements that can aid in surgical planning. The reconstructed 3D image allows an excellent overview of the craniofacial skeleton that serves as a useful tool for both planning the corrective surgery, as well as for intraoperative reference. These image files can also be used for virtual surgical planning and 3D printing of osteotomy guides and occlusal splints, should the surgeon choose to pursue that option.
Plain films are of little use in these cases, as the resolution is suboptimal for accurately visualizing fractures in the context of the complex craniofacial skeleton. However, a panoramic radiograph (panorex) can be helpful specifically in the setting of dental trauma, as it does provide an accurate view of the teeth and related deformities.
Case Examples
Case 1
This woman had a sagittal split osteotomy done elsewhere, and ended up losing full-thickness mandible from the right parasymphyseal area to the subcondylar area. She was treated with a fibular free flap extending into the glenoid fossa, another sagittal split with mandibular advancement on the left side, and a genioplasty ( Figs. 3.9.1 and 3.9.2 ).




Case 2
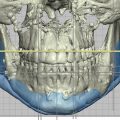
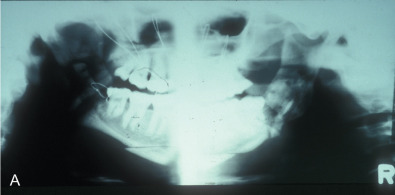
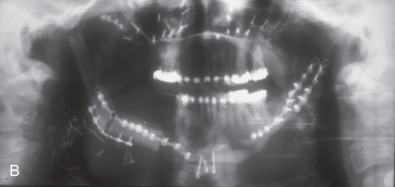
This man sustained a Le Fort I fracture during the Iran/Iraq war, was taken prisoner, and the fracture went untreated. When first seen he had no nasal airway, and the maxilla was very retruded and vertically impacted ( Fig. 3.9.3 ). The Le Fort I osteotomy performed on him was difficult since the pterygoid plates had been fractured, and it was very hard to get the maxilla adequately mobilized. This was eventually accomplished, but the usual medial and lateral buttresses were not present for rigid intersegment fixation. The one remaining maxillary tooth, a right first bisucpid, was advanced in front of the mandibular right cuspid, and a long 2.0 mm miniplate was fixed to the infraorbital rim with several screws (through a small infraorbital incision), fixed to the edentulous alveolar ridge and palate, and extended to the mandibular symphysis where it was fixed with several long 2.0 mm screws ( Fig. 3.9.4 ). The maxilla was lengthened vertically 21 mm; the amount of sagittal advancement was approximately the same (no cephalometric studies are available to quantitate this measurement precisely).