Secondary Deformities
Catharine B. Garland
Jesse Goldstein
Joseph E. Losee
DEFINITION
After cleft lip and nose reconstruction, secondary deformities of the lip and nose are common. The actual incidence of deformity is difficult to quantify because of individual variability in assessing what constitutes a deformity. For example, the incidence of revisionary surgery ranges from 0% to 100%.1
Asymmetries leading to deformity can be encountered anywhere along the lip-nose complex. These are caused by inadequate tissue in some cases and excessive tissue in others.
This chapter focuses on addressing secondary cleft lip deformities rather than secondary cleft rhinoplasty. Correcting asymmetries of the alar bases, however, is often an important component of secondary lip revision surgery.
ANATOMY
The ideal lip and nose complex is composed of the following features:
A symmetric nostril shape, with symmetric nostril sills and alar base position
A balanced Cupid’s bow with a smooth curve to the vermilion border
Symmetric philtral columns with a well-defined philtral dimple2
Smooth contour and balance of the mucosa
A central pouting tubercle in the vermilion
A functional orbicularis oris muscle sling that leads to symmetry with animation
Appropriate tooth show at rest
PATHOGENESIS
Some secondary deformities are intrinsic, such as the nasal deformity characterized by a hypoplastic and flattened lower lateral cartilage.
Other deformities are iatrogenic from the primary cleft repair. These include deformities caused by scarring, inadequate correction, an unbalanced reconstruction, or altered growth and development.
PATIENT HISTORY AND PHYSICAL FINDINGS
The most important part of the history is to ascertain what bothers the patient and the family. This may not always be congruent with what the surgeon sees as the most significant deformity. Realistic expectations of operative intervention must be discussed preoperatively.
The physical examination must include a careful analysis of the deformity. The reconstruction is then tailored to address the specific anatomic abnormality.
Are the alar bases symmetric in shape and position? They must be symmetric in the vertical, transverse, and sagittal plane.
What is the nature of the cutaneous scar? Assess whether the scar is hypertrophic, atrophic, or pigmented. This helps to inform the surgeon about the patient’s innate healing response.
Is the philtrum well defined and symmetric?
Is Cupid’s bow balanced or is there a discrepancy in height on the cleft side? Are the vermilion border and white roll congruous structures?
Is the red line, wet-dry junction, in alignment? An excess of wet mucosa in a region that should be composed of dry vermilion often causes persistent chapping of the lip in that area.
Is there adequate lip length and appropriate tooth show? Is the buccal mucosa scarred and tethered?
Is the mucosa symmetric? Is there excess mucosa on the cleft side or deficient mucosa at the central tubercle? Is there a notch in the mucosa at the site of repair?
Is the lip symmetric in animation? Bunching of the lip may suggest dehiscence of the orbicularis oris muscle.
SURGICAL MANAGEMENT
Preoperative Planning
Preoperative workup is per hospital routine.
Under anesthesia, a careful analysis of the lip and nose is again performed to characterize the asymmetries.
Positioning
Supine
We typically use an oral RAE endotracheal tube. This minimizes any asymmetry caused by taping a standard endotracheal tube in the corner of the mouth.
The table is turned according to surgeon preference.
The face is prepped with Betadine, and sterile drapes are applied. A head wrap or four towels may be used for draping according to surgeon preference.
Approach
Markings: Mark all the key anatomical landmarks of the lip and nose (eg, alar bases, columella, peak and nadir of Cupid’s bow, white roll, and wet-dry junction). Tattoo the key points with methylene blue.
Measure: Measure both the normal and cleft sides with calipers to determine the exact discrepancy of height and/or width in the lip and nose that requires correction.
Epinephrine: Consider whether epinephrine is needed for your surgery. The hemostatic benefit is helpful in many cases. However, for subtle contour abnormalities, epinephrine infiltration may obscure your ability to assess the result on the table. In these cases, pinch the lip between the thumb and index finger to occlude the labial artery while you are incising the tissues and use Bovie electrocautery sparingly.
Skin repair: Although hypertrophic scarring may be inherent to the patient, all precautions are taken to minimize this risk. Care is taken to ensure a tension-free closure. The skin is approximated with 5-0 or 6-0 Monocryl buried dermal sutures. When these are placed precisely, additional cutaneous sutures may not be required. When cutaneous sutures are needed, we use strategically placed 6-0 fast-absorbing plain gut or 6-0 nylon sutures in the epidermis to align the skin edge. These are removed 4 to 5 days after surgery.
Muscle repair: Muscular dehiscence may be suspected in patients who have a muscle bulge laterally with facial animation. In addition, muscular dehiscence can contribute to a shortened lip, notching of the mucosa, or widening of the cutaneous scar. When these are noted, reconstruction of the orbicularis oris musculature must also be performed with the repair. The orbicularis oris muscle is dissected free from the skin and mucosa. When the muscle is found dehisced, it is reapproximated or overlapped. Some surgeons describe a benefit to tightening the orbicularis oris muscle with horizontal mattress sutures to evert the muscle and accentuate the philtral column.
Mucosa repair: After the planned local tissue rearrangement or excision, the mucosa is typically repaired with 5-0 chromic gut sutures. These can be placed as everting horizontal mattress sutures to prevent a notch in the vermilion and mucosa.
TECHNIQUES
▪ Deformities of Cupid’s Bow
Small Vermilion Mismatch (Less Than 1 mm) or a Widened Scar at the Cutaneous-Vermilion Border
This can be managed by a diamond or curved excision of the scar, similar to the classically described Rose-Thompson straight line repair (TECH FIG 1A).
The Cupid’s bow nadir and high points are marked (TECH FIG 1B). An equal distance from high point to nadir is transposed to the cleft side, and this is typically positioned on the medial side of the scar. The vermilion border is marked medially and laterally to the scar that is to be excised. These points will come together to create the new high point of Cupid’s bow on the cleft side.
The white roll is marked, as is the red line wet-dry junction. The diamond excision is marked to excise the scar or mismatch and allow realignment of the vermilion border and white roll.
The critical points are tattooed with methylene blue.
Epinephrine-containing solution is infiltrated into the tissues for hemostasis.
Using an ophthalmic knife, the diamond is excised through the skin down to muscle. If the muscle repair is adequate, superficial scar is excised, but the muscle is left intact.
TECH FIG 1 • A. Hypertrophic scar at the vermilion border with slight shortening of Cupid’s bow on the cleft side preoperatively. The remainder of the cutaneous scar is well healed. B. The peak and nadir of Cupid’s bow are marked on the noncleft side and transposed to the cleft side. The white roll is marked and these points are tattooed. A diamond excision of the scar is marked at the vermilion border. C. The diamond excision realigns the vermilion border and white roll and provides adequate additional length to balance Cupid’s bow.
5-0 Monocryl is used to realign the vermilion border with a deep dermal suture (TECH FIG 1C). Additional deep dermal sutures are used to realign the wound margins precisely.
5-0 Chromic is used to reapproximate the mucosa with everting sutures. To prevent a standing cone or “dog ear,” excess mucosa is excised as needed in this process.
Cupid’s Bow Mismatch of 1 to 2 mm
For a Cupid’s bow mismatch of 1 to 2 mm (TECH FIG 2A), a small triangular flap is inserted at the cutaneous border.
This excision and reconstruction are often similar to the microform cleft repair described by Mulliken.4
The cutaneous-vermilion border, white roll, Cupid’s bow peak on the normal side, low point, and peak on the cleft side are marked and tattooed (TECH FIG 2B).
Using calipers, the distance from subnasale to the normal Cupid’s bow peak is measured, and the equal distance from subnasale is marked on the cleft side.
A laterally based cutaneous equilateral triangular flap is marked on the lip above the white roll, with the base of this triangle being the difference in the distance between subnasale and height of Cupid’s bow peak on each side.
An incision of equal length is marked on the medial lip element above the white roll.
The length of vertical excision is long enough to excise any abnormal scar tissue or to prevent formation of a “dog ear.”
If there is a deficiency of central tubercle vermilion, a laterally based triangle of vermilion may be designed as well.3 If there is an excess of lateral mucosa, a mucosal excision may be included (TECH FIG 2C).
The tissue is infiltrated with epinephrine. It is excised with an ophthalmic knife or no. 15 blade.
The scar tissue is excised and the skin flaps are separated from the underlying orbicularis oris muscle.
The muscle is reconstructed if needed, and skin and mucosa repair proceeds as previously described (TECH FIG 2D,E).
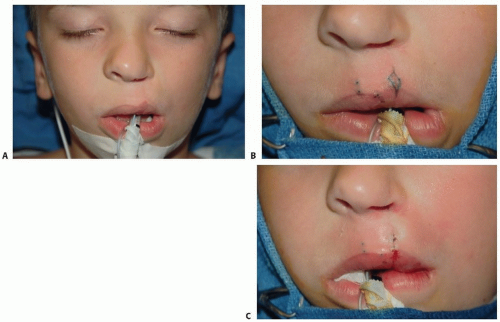
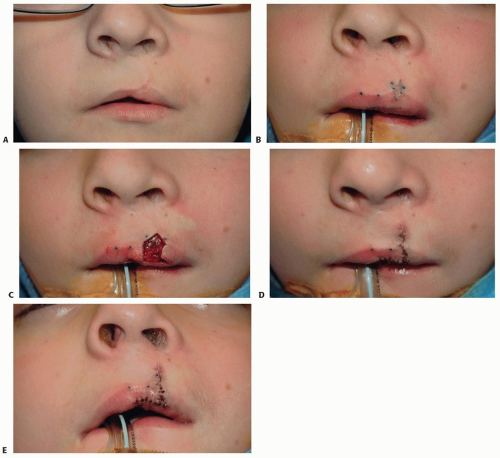 TECH FIG 2 • A. Lip deformity characterized by both shortening of Cupid’s bow on the cleft side and lateral mucosal fullness. B. The peak and nadir of Cupid’s bow are marked on the noncleft side, and the peak of Cupid’s bow is marked symmetrically on the cleft side. The excision is designed with a laterally based triangular flap at the white roll. In addition, the lateral mucosal fullness is addressed with an excision planned along the red line or junction of wet and dry mucosa. C. After excision of the tissues, prior to repair. Mucosa is being excised in both the transverse and vertical planes. D. Closure includes the inset of a laterally based triangular flap above the white roll to increase the length of the lip on the cleft side. This realigns and balances Cupid’s bow. E. After excision of excess mucosa, the mucosa is more symmetric. The scar is hidden along the red line and closed with 5-0 chromic sutures. |
Cupid’s Bow Asymmetry More Than 2 mm High
For a larger asymmetry, a complete revision of the cutaneous scar is performed (TECH FIG 3).
Many primary lip repair techniques may be adapted to achieve the necessary goals in these more complex deformities.
The vermilion discrepancy may be addressed by rerotation of the medial lip element as in a classic Millard repair (TECH FIG 3C).
Use of a triangular flap above the white roll in the manner first described by Tennison and Randall and subsequently modified by Fisher5 is also an option for a complete revision of the lip repair to address a major deformity.
The orbicularis oris muscle may need to be reconstructed fully or in part to achieve adequate repair.
In the bilateral cleft lip, complete revision is used for patients with a wide philtrum, significant philtral scarring, or a severe deficiency of vermilion in the midline (TECH FIG 4).
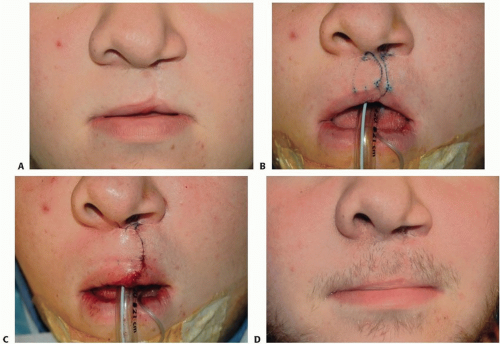 TECH FIG 3 • A. Shortening of the unilateral lip with mild widening of the cutaneous scar. B. A complete excision of the cutaneous scar is planned. A backcut is designed to allow secondary rotation of the medial lip element. C. After rotation of the medial lip element, Cupid’s bow is now more symmetric. D. The improvement in the symmetry of Cupid’s bow is maintained at 18 months postoperatively. |
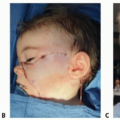
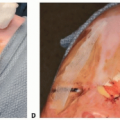
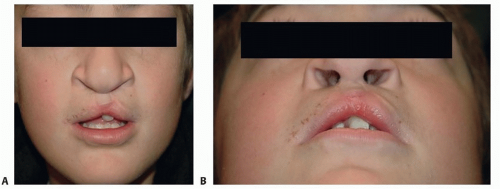 TECH FIG 4 • A,B. A 12-year-old boy with significant residual cleft lip and nasal deformity after bilateral lip repair. Cupid’s bow is unbalanced, and there is a paucity of mucosa in the central tubercle. He has had no correction of his cleft nasal deformity with lateral displacement of the alar bases. |
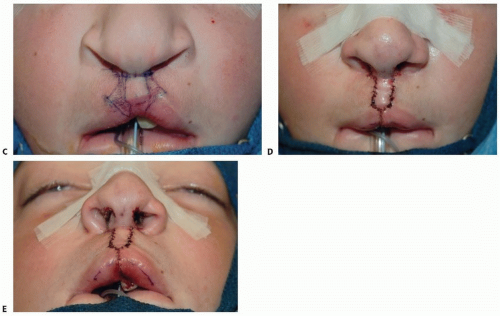 TECH FIG 4 (Continued) • C. With this degree of deformity, a complete bilateral lip and nose repair is planned and marked as if this were a primary incomplete bilateral lip repair. The peak of Cupid’s bow is marked at Noordhoff point on the lateral lip element. The skin and mucosa between this and his existing scar are planned for excision. D,E. The bilateral lip and nose are completely reconstructed to restore balance to Cupid’s bow and the vermilion. Note the improved positioning and symmetry of the lower lateral cartilages and alar bases after open reconstruction with inverted-U rim incisions to address the lower lateral cartilages. |
▪ Abnormalities of the Vermilion and Mucosa
Minor notches in the vermilion, asymmetries of the mucosa, incongruity of the red line, or asymmetry of the dry vermilion may all be managed with small elliptical excisions or local tissue rearrangement.
Incisions are confined to the mucosa and vermilion unless a cutaneous deformity must also be addressed.
Each problem discussed here has a slightly different solution, but our typical step-by-step approach is as follows:
Assess the deformity and design the excision or flap for reconstruction.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree