The primary lesion of a papulosquamous disorder is a papule with scale, but because patients often present later in the course of disease, the primary lesions may not be visible, and the physician may observe scaly plaques, patches, postinflammatory change, or diffuse redness and scaling (erythroderma).
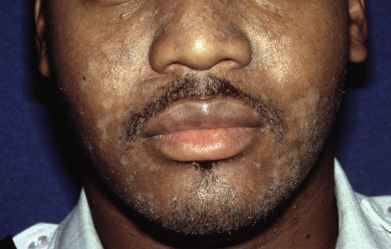
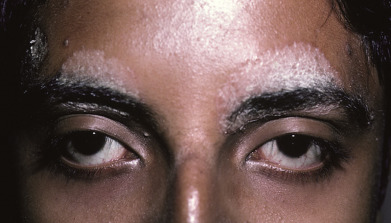
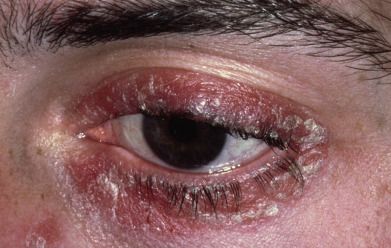
Seborrheic dermatitis may involve the eyebrows, nasolabial and melolabial folds, scalp, ears, retroauricular regions, central chest, and axillae. The scale often exhibits a yellow hue, most likely related to carotenoids within the serum crusts. This is in stark contrast to the silvery white scale of typical plaque psoriasis. Plaque psoriasis lacks spongiosis (and the yellow carotenoids that are dissolved in the aqueous phase of tissue fluids). Several forms of psoriasis exhibit spongiosis and can sometimes have a slightly yellow appearance to the scale. These include guttate, inverse, acral, and erythrodermic forms of psoriasis. Even in these forms, frankly yellow scale and honey crusts are rare.
Erythroderma presents with generalized erythema and scaling. Edema may be present, especially involving the face and extremities, and patients may suffer chills as a result of loss of body heat. Older patients may exhibit signs of high-output cardiac failure. This portion of the atlas will guide you through the various clinical manifestations of seborrheic dermatitis, psoriasis, and related disorders.






















Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


