8.7 Sculpted pillar vertical reduction mammaplasty
Synopsis



Planning and markings
 Video 1
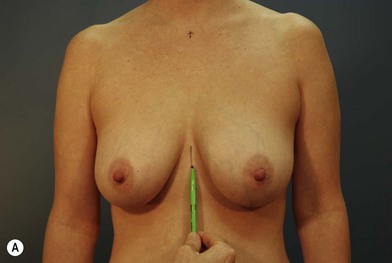
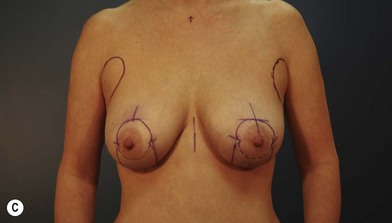
Video 1The markings are performed with the patient in the standing position (Fig. 8.7.1). The future nipple position is determined right at the reflection of the inframammary fold on the anterior surface of the breast (the A-point or Pitanguy point). This is checked against the visual midpoint of the acromion to humerus distance, as well as other visual landmarks. Typically, this point is about 2 cm lower than the point chosen for inverted T techniques. It is preferable to use the standard superior pedicle for the nipple-areolar complex, but if the density of the gland or distance of elevation appears restrictive, the superomedial pedicle recommended by Hall-Findlay is used.1,2 The medial and lateral pillar lines are drawn by manually distracting the breast tissue medially and laterally. The volume to be left behind is approximated, and the resulting shape is visualized (Fig. 8.7.2). These lines should anticipate the parenchyma to be removed and should be adjusted in or out on the basis of the planned volume of resection. These lines mark the anterior-most projections of what will be, after resection of the intervening parenchyma, the vertical pillars of this technique. Inferiorly, the bottom of the V should be at least 2–3 cm above the native inframammary fold (Fig. 8.7.3). It is also preferable to mark on the skin surface the glandular tissue that will be resected at the caudal extent of the planned medial and lateral pillars, much the same way as one would mark this in a Wise pattern reduction. This will indicate the level of base resection for the medial and lateral vertical pillars, which, when approximated later in the procedure, will stabilize the construct of the new breast on the chest wall via these adjoined medial and lateral solid pyramids.






 Video 2
Video 2








