Scalp Reconstruction With Rotation Flaps
Finny George
Evan Matros
DEFINITION
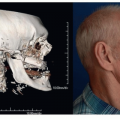
The scalp serves as a protective layer for underlying deep structures including the calvarium and brain.
It plays an equally important aesthetic role in providing hair coverage.
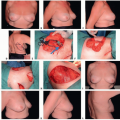
Rotation or local flaps can be useful in reconstructing defects up to 5 cm and can be utilized first, before ascending the reconstructive ladder.
Replacing like tissue with like tissue results in superior results both aesthetically and functionally, particularly with regard to the presence or absence of hair.
Adequate scalp compliance and pliability is necessary to effectively rotate adjacent scalp tissues.
Patients with tight scalp tissues or those with radiationor surgery-induced fibrosis will have less pliability and rotation potential. The use of scalp flaps in these patients, as well as those with locally aggressive pathology, exposed hardware, and potential exposure of underlying tissues, may be limited.
ANATOMY
The layers of the scalp are the skin, subcutaneous network (contains blood vessels, lymphatics, and nerves), galea aponeurotica, areolar plane, and pericranium.1
The skin of the scalp is the thickest of all the skin on the body.
Vertical septa connecting the galea to the skin minimize shearing.
The galea is a fibromuscular central tendinous confluence of the occipitalis and frontalis muscles. It is contiguous with the superficial temporal fascia and the SMAS.
The loose areolar plane is the layer in which separation of the scalp from the cranium occurs during trauma. This property can be used during reconstructive surgery to obtain soft tissue advancement.
The parietal scalp has the greatest mobility and can be helpful in local tissue recruitment.
Vascular supply
The principal blood supply is the supraorbital, supratrochlear, superficial temporal, occipital, and posterior auricular vessels.
The vascular supply is derived from both the internal and external carotid systems and forms a rich collateral network. For example, an entirely avulsed scalp can be replanted after repair of only one major blood vessel.
Sensory
The trigeminal nerve contributions are as follows:
Supraorbital and supratrochlear nerves supply the forehead, anterior hairline, and frontoparietal regions.
Zygomaticotemporal and auriculotemporal nerves supply the temporal region.
The occipital and greater occipital nerves supply the occipital region. These originate from the cervical spinal nerve and plexus.
PATHOGENESIS
Defects of the scalp often result from trauma, malignancy, or congenital disease.
Radiation damage creates two potential reconstructive dilemmas. Radiation can cause chronic wounds. It also limits soft tissue compliance for defect closure.
Underlying calvarial reconstruction with a cranioplasty introduces a foreign body and hardware, which can be a chronic wound source.
PATIENT HISTORY AND PHYSICAL FINDINGS
Pertinent history must include information on:
Circumstances surrounding injury
If the pathology is secondary to tumor excision, then margin status, potential for local or systemic dissemination, should be documented. Ideally, reconstruction should be delayed until negative margins are obtained; however, this is not always possible when vital structures or hardware is exposed.
Prior treatment or operations that were done, including failed treatments
Underlying presence of hardware or implants
History of radiation or chemotherapy, immunosuppression, or connective tissue disorders.
History of smoking, alcohol abuse, weight loss, diabetes, or bleeding disorders should be documented.
Physical examination should gather enough knowledge to prepare an accurate preoperative plan.
Look for prior incisions, evidence of poor wound healing, and radiation changes (eg, woody, discolored skin with telangiectasia).
Examine the skin laxity.
Available remaining blood supply to the scalp especially in the setting of prior surgery
Areas of numbness should be documented.
Doppler examination may be helpful to document course and integrity of arterial supply.
Chronic wounds should be biopsied to rule out recurrent, residual, or new malignancy.
IMAGING
Diagnostic studies are typically not needed for reconstructive surgery planning; however, these may be necessary for oncological analysis.
NONOPERATIVE MANAGEMENT
In poor surgical candidates, nonoperative or conservative management may be possible so long as there is no direct communication with the brain.
This option is best reserved for patients in whom the calvarium is intact and has not been previously injured by radiation or surgery.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree