Local Flaps in Partial Breast Reconstruction
Moustapha Hamdi
Fadi Bakal
DEFINITION
Partial breast reconstruction is an area of evolving interest with improving surgical techniques; it is indicated in breast conservation therapy (BCT), which is on its own a popular treatment option for women with breast cancer.1,2 The rate of its use has increased from 40% in 1991 to 60% in 2002 when compared with mastectomy, and that trend continues to rise.1
Oncoplastic surgery within multidisciplinary approach is standard in BCT.
The oncoplastic surgical approach allowed surgeons to tailor the techniques to prevent deformities, minimize involved margins, and reduce the potential for local recurrence.
Partial breast reconstruction with pedicled flap is alternative to mastectomy in selected patients as such in patients with a high tumor/breast size ratio.
Every case requiring partial breast reconstruction should be addressed within a multidisciplinary approach.
Pedicled perforator flaps provide adequate partial breast reconstruction with minimal donor-site morbidity.
ANATOMY
The latissimus dorsi (LD) flap has a constant anatomy.3,4,5 The blood supply of the latissimus dorsi comes from a terminal branch of the subscapular artery. The subscapular artery runs about 5 cm before dividing into the scapular circumflex and thoracodorsal arteries.
The thoracodorsal artery gives off one or two branches to the serratus anterior muscle and one branch to the skin (FIG 1).
PATIENT HISTORY AND PHYSICAL FINDINGS
Breast and plastic surgeons must have a thorough understanding of breast anatomy and physiology and the qualities of an aesthetically pleasing breast shape.
Surgeons performing the oncoplastic approach should consider the aesthetic subunits when planning cosmetic quadrantectomies, resections, and reconstructions.3
Also, knowledge of the anatomical landmarks, breast proportions, and shape is essential to achieve a pleasing outcome.
Preoperative evaluation of the patient and her breasts must be standardized and detailed.
The examination must include the following:
Evaluation of breast skin, elasticity, thickness, scars, and any defining marks such as tattoos, stretch marks, contour irregularities, and previous breast surgery should be taken into account when planning BCT.
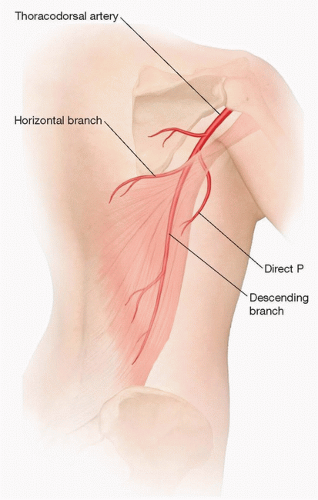
FIG 1 • The TD vessels most commonly divide into five branches, but two are dominant muscular branches: the transverse branch, and the lateral or vertical branch. Both branches give musculocutaneous perforator to the skin. A direct branch can also be found, which courses anteriorly around the LD muscle toward the skin.
Palpation for masses or abnormalities in the breast parenchyma, nipple inspection, and detailed documentation of breast sensation are integral.
Breast shape, grade of ptosis, and size are determinants of success in surgical treatment.
The base and width of the breast, the width of the NAC, the height of the nipple, and the distance from the sternal notch, midline, and inframammary crease must be recorded in detail.4
Any natural breast asymmetry should be pointed out to the patient before surgery.
Different body types, skin laxity, and fat distribution are important factors in the decision-making process.
SURGICAL MANAGEMENT
Depending on the location and the size of the breast defect, different flaps can be used for partial mastectomy reconstruction based on the thoracodorsal-serratus, intercostal, or superior epigastic vessels.2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18
A small lateral defect can easily be closed with a skin rotation flap or lateral thoracic axial skin flap. However, most of these flaps become unavailable when axillary lymph node dissection is performed.
Lateral breast defects are usually reconstructed using a flap based on the thoracodorsal system. The LD musculocutaneous flap is the most commonly used.
Currently, perforator flaps are more often used to spare muscle function.
The pedicled perforator flaps mostly used by us for partial breast reconstruction, classified according to the basic nutrient arteries and recommended by the “Gent” Consensus update in 2002,6 are

FIG 2 • Illustrations show: TDAP flap with musculocutaneous perforators (A).
Thoracodorsal artery perforator (TDAP) flap
Serratus anterior artery perforator (SAAP) flap
Intercostal artery perforator (ICAP) flap
Superior epigastric artery perforator (SEAP)
A similar skin paddle to the classical LD musculocutaneous flap can be raised on perforators either from the thoracodorsal or intercostal vessels.
Types of Flaps
TDAP Flap
The TDAP flap is based on perforators originating from the descending (vertical) or horizontal branches of the thoracodorsal vessels (see FIG 1; FIG 2). Anatomic studies on cadavers have reported the presence of 2 to 3 musculocutaneous perforators from the vertical branch.7,8,9
The proximal perforator enters the subcutaneous plane obliquely 8 to 10 cm distal to the posterior axillary fold and 2 to 3 cm posterior to the anterior border of the muscle. The second perforator is found 2 to 4 cm distally to the first one.
Occasionally, a direct cutaneous perforator arising from the thoracodorsal vessel passes around the anterior border of the muscle, making flap harvesting easier (see FIG 1).
There may not be always a single reliable perforator for the TDAP flap, due to anatomical variations. In this case, the surgeon must be aware and prepared to modify the flap dissection intraoperatively, as a muscle-sparing TDAP flap.
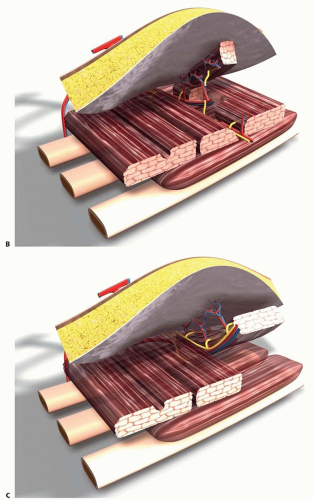
FIG 2 (Continued) • B. TDAP flap with perforator still attached to 4 × 2 cm muscle segment (muscle-sparing TDAP type I). C. TDAP flap raised on the descending branches and its perforators (muscle-sparing TDAP flap type II). Reprinted from Hamdi H, et. al. Pedicled perforator flaps in breast reconstruction: a new concept. Br J Plast Surg. 2004;57(6):531-539, with permission from Elsevier.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access






