Free Fibula Flap for Midface Reconstruction
J. Rodrigo Diaz-Siso
Eduardo D. Rodriguez
DEFINITION
Composite midface defects, involving skin, bone, and mucosa, are commonly the result of oncologic resection, high-energy trauma, inflammatory diseases, or congenital anomalies.
Unreconstructed midface defects may lead to impaired speech, oral incompetence, and limited masticatory, deglutitive, orbital, and respiratory functions, in addition to facial disfigurement and associated decreased quality of life.
The free fibula is a versatile flap that can include a long segment of vascularized bone, which can be shaped as needed through multiple osteotomies.
The flap can include muscle, fascia, and/or skin, making it an ideal reconstructive option for composite defects.
The reconstructive goals are to replace the facial buttresses, resurface internal and external soft tissue lining, separate the oral and nasal cavities, and restore the alveolus, resulting in a patent nasal airway, adequate midfacial projection and ocular globe position, and allowing for endosseous dental rehabilitation.
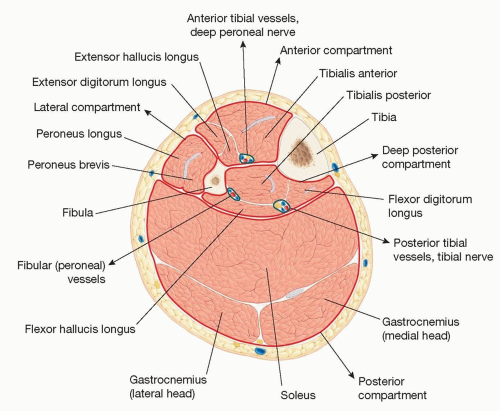 FIG 1 • Cross section of the middle leg showing fascial compartments and relevant anatomical structures. |
ANATOMY
The skeletal foundation of the lower leg is composed of the tibia (medial) and fibula (lateral), parallel long bones connected by an interosseous membrane, which divides the leg into anterior and posterior compartments (FIG 1).
The anterior compartment is bordered laterally by the anterior intermuscular septum. The anterior tibial vessels and deep peroneal nerve are directly anterior to the interosseous membrane.
The lateral compartment, which includes the peroneus longus and peroneus brevis muscles, is bordered posteriorly by the posterior intermuscular septum, which contains the perforator vessels that perfuse the lateral skin of the lower leg, and thus the skin island of the flap when applicable.
The deep posterior compartment includes, from medial to lateral: flexor digitorum longus, tibialis posterior, and flexor hallucis longus muscles; the fibular vessels run between the latter two. The posterior tibial vessels and tibial nerve are found lateral to the flexor hallucis longus, posterior to the tibialis posterior muscle, and anterior to the transverse intermuscular septum.
The posterior compartment includes the soleus and gastrocnemius muscles.
The fibula is nonweight bearing, but the proximal and distal epiphyses are crucial to the integrity and stability of the knee and ankle joints, respectively.
The common fibular nerve wraps around the neck of the fibula before dividing into the deep and superficial fibular nerves, limiting proximal dissection and procurement. Even after epiphyseal preservation, approximately 25 cm of vascularized bone can be harvested.
The fibular artery provides the dominant blood supply to the fibula, supplemented by periosteal and muscular branches; the vascular pedicle can be considerable, yielding up to 15 cm. The well-defined vascular supply allows the division of the free fibula into segments as small as 2 to 3 cm.
The two venae comitantes of the fibular artery are responsible for venous drainage.
The lateral sural nerve supplies the sensory innervation of the lateral leg skin; sensory nerve coaptation is possible, but not routinely performed.
Muscles commonly included in a free fibula flap include the flexor hallucis longus and the tibialis posterior, located in the deep posterior leg compartment. The soleus, located directly posterior to the posterior and transverse intermuscular septa, can also be included.
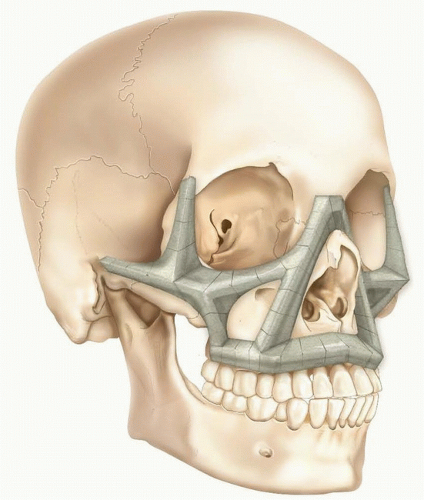
FIG 2 • Illustration of the horizontal and vertical skeletal buttresses of the midface.
Vertical: The nasomaxillary, zygomaticomaxillary, and pterygomaxillary buttresses maintain facial height and resist occlusal load.
Horizontal: The inferior orbital rim maintains the position of the ocular globe, and together with the maxillary alveolus and the malar prominence, it is responsible for maintaining the facial profile and width, respectively.
A classification of skeletal midface defects focuses on the absence of these essential functional subunits of the maxilla2 (FIG 3):
Class I: unilateral dentoalveolar defect
Class II: unilateral dentoalveolar and orbital rim defect
Class III: bilateral dentoalveolar defect
Class IV: bilateral dentoalveolar and orbital rim defect
Depending on concomitant skin deficits, and/or pterygoid injury, which affects the complexity of the posterior fixation of the flap, this classification is designed to determine flap selection for microsurgical reconstruction.2
Important: instead of attempting to recreate the absent curvilinear structures of the facial skeleton, segments of vascularized bone are strategically placed to serve as girders that are capable of (and necessary for) preserving function and maintaining aesthetic facial proportions and contour.3
PATIENT HISTORY AND PHYSICAL FINDINGS
A detailed medical history must be performed to identify patients with current or prior peripheral vascular disease, deep vein thrombosis, vasculitis, or lower leg trauma, which may increase the risk of an unreliable fibular vascular pedicle.
The popliteal, dorsalis pedal, and posterior tibial pulses are examined.
Lower extremity Allen test can be performed to ensure that both the dorsalis pedis and posterior tibial arteries perfuse the distal lower extremity.
The range of motion and stability of the knee and ankle joints are assessed.
Facial anthropometrics are assessed, including horizontal thirds and vertical fifths.
Dental/facial midlines, dental show at rest and smiling, and maxillomandibular occlusal relationships are recorded when applicable.
IMAGING
Angiography is not routinely performed but can be considered if history is positive for possible tibial artery damage or injury, and/or if distal pulse assessment is abnormal or suspicious.
Other imaging modalities (CT or MR angiography) are also effective alternatives.
In traumatic defects, three-dimensional maxillofacial CT will allow precise analysis of the missing bone that will be reconstructed, in addition to soft tissue analysis.
When computerized surgical planning (CSP) is employed, three-dimensional lower leg- and maxillofacial CTs are performed to aid the design of the flap, which is based on an existing traumatic defect or the predicted absent maxillary bone that will result from planned ablative surgery.
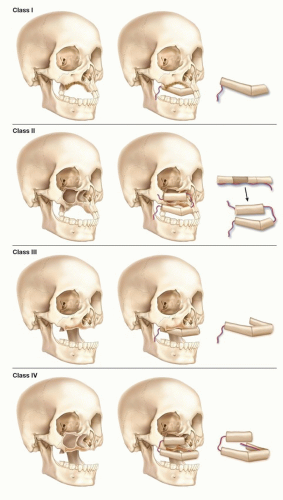 FIG 3 • Classification of midface skeletal defects in ascending order of reconstructive complexity, and illustrations of possible free fibula flap reconstruction of each defect. Class I: Unilateral dentoalveolar defect. Class II: Defect involves inferior orbital rim and ipsilateral maxilla. Class III: Bilateral dentoalveolar defect. Class IV: Defect involves bilateral dentoalveolar loss and at least one orbital rim. |
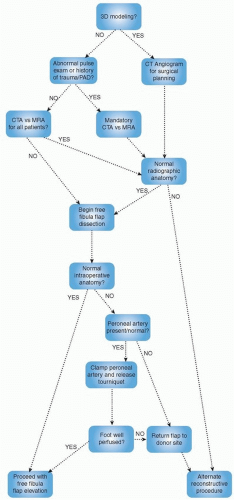 FIG 4 • Algorithm to rule out aberrant lower extremity vascular anatomy in a free fibula flap reconstruction candidate. |
NONOPERATIVE MANAGEMENT
Prosthetic obturation is among the earliest techniques developed to reconstruct facial defects.
Midfacial prostheses can be considered in patients who are poor candidates for—or unwilling to pursue—free tissue transfer.
Advanced age, medical comorbidities, smokers, contaminated wounds, etc.
In pediatric patients, prosthetic obturation can serve as a temporary reconstructive solution during growth.
Permanent free flap reconstruction can be revisited once the patient reaches skeletal maturity.
SURGICAL MANAGEMENT
Reconstruction of composite midface defects may not be possible in a single stage; surgical plans and patient expectations must be managed with this in mind.
Phase 1 goals: restore skeletal anatomy, eliminate dead space if necessary, and deliver soft tissue volume in slight excess for future refinement.
Consider early involvement of dental colleagues:
Close collaboration and detailed planning of osseointegrated implant placement is essential to optimizing dental rehabilitation and long-term outcomes.
Preoperative Planning
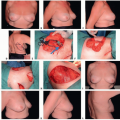
VSP can accurately predict and facilitate fibular osteotomy and flap inset sites based on 3D reconstructions of CT data (FIG 5).
3D-printed osteotomy guides ensure maximal precision during separation of the fibular segment from the lower leg, division of the bone flap into multiple segments, and fixation of the resulting segments to accommodate a desired flap shape.
VSP also identifies the best point of fixation on the midface, in addition to aiding the design of recipient-site osteotomies that may be required prior to optimal flap inset and fixation.
A 3D-printed model of the patient’s skull and the desired shape of the bone segment(s) help preoperative contouring of a 2.0-mm titanium miniplate, minimizing ischemia time. If required, minor adjustments in the shape of the plate can be made prior to flap inset.
Alternatively, stereolithographic models of the patient’s facial skeleton and remaining dentition can be used intraoperatively for this purpose.
Preferred recipient pedicles are the superficial temporal and facial vessels.
Unilateral defects: whenever possible, ipsilateral vessels are preferred.
Bilateral defects: less relevant; will depend on quality of local tissues; may determine recipient site selection.
Class IV defects (bilateral dentoalveolus and inferior orbital rim): multiple free flaps may be indicated; bilateral recipient vascular pedicles will likely be necessary.
When choosing between ipsilateral and contralateral donor fibula, consider the following:
The fibular vessels are located on the medial surface of the fibula, and the flap’s vascular pedicle extends superiorly from the proximal end of the procured bone segment.
Thus, the fixation plates will be screwed onto the lateral surface of the fibula, which will become the anterior surface of the reconstructed midface bone (flap vasculature will run on posterior surface).
Recipient vessel selection may be limited in extensive defects, and vascular compromise of one leg may force the surgical team to procure the flap from the opposite side. Nevertheless, fibula flaps can be rotated 180 degrees to reach ipsilateral or contralateral recipient vessels depending on reconstructive needs.
A fibula flap ipsilateral to the chosen recipient vessels may be oriented more easily so that, upon inset, the donor
vascular pedicle does not cross the midline to reach the recipient vessels.

FIG 5 • Computerized surgical plan to reconstruct a midface defect that resulted from the resection of a right maxillary oncologic deformity in a 58-year-old man. A. Synthes ProPlan software was used to calculate the overall length of the fibula segment to be elevated, as well as the length of each fibula segment to be osteotomized and reshaped before flap inset. B. Patient’s preoperative anatomy showing the right maxillary defect, and the virtually planned postoperative result with the fibula segments recreating the horizontal maxillary buttresses.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access