Lower Eyelid Reconstruction With Palatal Grafts
Farooq Shahzad
Babak J. Mehrara
Aaron Fay
DEFINITION
With proper case selection, lower eyelid reconstruction can be enhanced using hard palate grafts.
Both horizontal deficiency and vertical retraction can be corrected using this technique.
Palatal grafts are not suitable for upper lid reconstruction because the keratinized surface can abrade the underlying cornea.
ANATOMY
Eyelids
For purposes of reconstruction, it is useful to consider the eyelids in three constituent layers, or lamellae: anterior, middle, and posterior (FIG 1). Below the lid crease in the region of tarsus, only anterior and posterior layers can be defined.
The anterior lamella comprises skin and orbicularis oculi muscle. Eyelid skin is the thinnest in the body, entirely lacking subcutaneous fat. This makes skin matching difficult when placing full- or split-thickness skin grafts. Whenever possible, eyelid skin grafts are harvested from the contralateral or opposing eyelids.
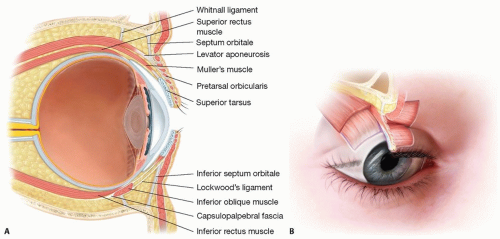
FIG 1 • A. Sagittal section through superior eyelid showing lamellar anatomy. Below the lid crease, the anterior and posterior lamellae are well defined. Anterior lamella consists of skin and muscle, while posterior lamella consists of tarsus and conjunctiva. Above the lid crease, three layers of lid are recognized: conjunctival and retractor muscles constitute the posterior layer, orbital fat and septum constitute the “middle lamella,” and skin and muscle constitute the anterior lamella (extension of SMAS onto the eyelid). B. Anterior view of eyelids demonstrates the normal contour and resting position of the upper and lower lid margins. Note that the superior limbus and inferior limbus are concealed by the upper and lower lid margins, respectively.
The lashes arise in the anterior lid margin and project anteriorly and superiorly in the upper lid. In the lower lid, the lashes are less robust, projecting anteriorly and inferiorly. Lamellar disjunction can produce eyelash ptosis that interferes with vision.
Orbicularis oculi is a thin, circumferential striated muscle that can be conceptualized in three regions: pretarsal, preseptal, and orbital. Pretarsal orbicularis extends all the way to the lid margin, where it can be visualized as the “gray line” separating anterior and posterior lamellae. This important landmark is known as the muscle of Riolan. Responsible for blinking, the preseptal orbicularis extends from the tarsal periphery (superior edge or inferior edge of tarsus in the upper or lower eyelids, respectively) approximately to the level or arcus marginalis around the orbital rim. When stimulated, this portion of orbicularis produces complete, intentional, mildly forceful closure with no radial rhytide formation, as used, for example, upon sleeping. Preseptal orbicularis stimulation is usually accompanied by a Bell phenomenon (upward rotation of the eyeball). The orbital portion of orbicularis oculi extends peripherally
beyond the arcus marginalis and eventually interdigitates with frontalis and corrugator muscle superiorly. This portion of muscle produces tight, forceful eyelid closure accompanied by glabellar and lateral rhytide formation. Orbicularis oculi originates and inserts along the raphe near the medial and lateral canthi.
The middle lamella, distinguishable only superior to the primary upper lid crease (and inferior to the tarsus in the lower eyelid), consists of a fibrous orbital septum and orbital fat. The orbital septum originates at the arcus marginalis along the superior orbital rim and inserts onto the distal aponeurosis of levator palpebrae superioris. This plane defines the anterior limit of the orbit; the skin and orbicularis represent the terminal extension of the frontal SMAS, whereas retroseptal tissues (levator muscle, Muller muscle, and conjunctiva) originate deep within the orbit. These distinctly different planes fuse along the orbital septum, the “periosteum” of the eyelid.
The posterior lamella consists of the conjunctiva, tarsus below the lid crease, and eyelid retractors above the lid crease. Levator palpebrae superioris (levator muscle) and Muller muscle (sympathetic eyelid muscle) form the upper eyelid retractors. In the lower lid, these muscles fuse more completely, the so-called capsulopalpebral fascia. All structures in the upper lid have analogues in the lower eyelid. Formed of collagen (not cartilage), the tarsal plates are the structural elements of the eyelid, lending rigidity, stability, and directionality especially to the lid margin regions. The center of the upper and lower lid tarsi are approximately 10 and 4 mm high, respectively. These structures taper laterally and medially where they fuse with medial and lateral canthal tendons. Because they taper quite significantly, direct closure of tarsal defects produces mismatched tarsal elements; the lid margin provides a template for reconstruction.
The medial canthal tendon inserts on the medial orbit via two crura, along the anterior and posterior lacrimal crest. During reconstruction, it is important to reconstitute the posterior crus so that the lid hugs the ocular surface all the way to the caruncle. Without it, the lid can become distracted anteriorly, leaving a space between the lid margin and ocular surface. The lateral canthal tendon inserts on the periorbita of the lateral orbital tubercle of Whitnall posterior to arcus marginalis. Here again, it is important to reattach the tendon posteriorly in order to draw the lid tightly against the globe all the way to the commissure, particularly in deep-set eyes and, less importantly, in relatively proptotic eyes.
Upper eyelid contour forms a smooth, continuous arc with its apogee typically at the medial pupil. The upper eyelid margin typically conceals 2 mm of superior cornea, whereas the lower lid sits at or just above the inferior corneal limbus. These measures should be evaluated with the patient’s head in neutral position, as chin-up or chin-down positioning will dramatically alter the lower lid position. Simultaneous unveiling of the superior and inferior limbus produces a “Walt Disney eye,” characteristic of thyroid eye disease. An imaginary line segment connecting the medial and lateral canthi is slightly canted upward and outward in most patients, the positive canthal tilt. During reconstruction, the lateral canthus should be placed approximately 2 mm superior to a horizontal line drawn through the two medial canthi.
The blood supply to the eyelid forms anastomoses between internal and external carotid artery circulations through the marginal and peripheral vascular eyelid arcades extending across the eyelids. The external carotid circulation progresses medially through the facial artery and then the angular artery and laterally through branches of the superficial temporal artery. Supraorbital, supratrochlear, and infraorbital branches from the ophthalmic artery form the internal carotid contribution.
Hard Palate
The hard palate separates the oral and nasal cavities. The anterior three-fourths is formed from the horizontal process of the maxilla, whereas the posterior portion consists of horizontal portion of the palatine bone. The anterior and lateral periphery of the palate is known as the alveolar arch. Posteriorly, the hard palate is continuous with the soft palate.
The mucosa of the hard palate is tightly bound to the periosteum by a surprisingly thick fibrous submucosa. The midline mucosal ridge is called the palatine raphe (FIG 2).
The blood supply of the hard palate is via the greater palatine artery that exits the greater palatine foramen medial to the 3rd molar. This vessel travels anteromedially and enters the incisive foramen in the anterior palate. The greater palatine nerve travels with the artery.
PATIENT HISTORY AND PHYSICAL FINDINGS
History
Historical visual acuity is obtained to help determine visual potential in the eye. History of dry eye or other ocular pathologies should be obtained, with ophthalmic consultation as indicated.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree