5Scalp
Abstract
Scalp reconstruction is commonly required after Mohs surgery. Creative use of a broad range of reconstruction options rewards both physician and patient with excellent cosmetic and functional outcomes. Excellence requires complete understanding of the anatomy of the scalp, including the location of multiple neurovascular bundles, and an appreciation of how the convex surface and relatively thick, poorly mobile skin make reconstruction challenging. Defect size, location, and presence or absence of hair or periosteum are important decision points when choosing a reconstructive option. Answers to these questions, when combined with patient factors (medical history, cosmetic desires, ability to care for the surgical site), allow the surgeon to develop a reconstruction ladder and algorithm. Second intention healing is useful for defects, even those without periosteum, in a range of defect sizes, in appropriate appropriately selected. Skin grafts, both full thickness and split thickness, are reserved for moderate to large defects in alopecic scalps when intact periosteum is present. In patients who are not able to care for a graft donor site, allogenic materials can serve as graft substitutes. The usefulness of primary closure can be extended to large defects by combining with pulley or purse-string sutures. Local flaps, either single or multiple, are a mainstay reconstruction option as they provide similar tissue and a secondary defect, which can be easily closed. Extensive defects not suitable for second intention healing or grafting require referral for placement of an internal tissue expander or consideration of free autologous tissue transfer.
Keywords: scalp, reconstruction, anatomy, second intention healing, skin grafts, autologous skin substitutes, local flaps, pulley sutures, purse-string sutures, free tissue transfer
Capsule Summary and Pearls
•The majority of undermining is at the subgaleal plane to minimize damage to overlying blood vessels, lymphatics, and nerves.
•Scalps have both tight and loose portions. Tight areas over the scalp vertex occur where the galea is thickest. Loose areas over the scalp periphery, especially occipital and parietal scalps, occur where the galea is less developed and blends with fascia of the scalp muscles.
•Second intention is a viable reconstructive option for scalp defects, especially if the scalp has had prior surgeries or a high-risk cancer requires close surveillance for recurrence.
•Second intention healing over bone is possible but requires prolonged and meticulous wound care in a moist environment.
•Mid-dermal placement of local anesthetic is most efficient and effective but requires high injection pressures.
•Anesthetic can be injected into the planned incision lines and standing cones while leaving the rest of the area to be bluntly undermined in the painless subgaleal plane.Galeal releasing incisions reduce tension only minimally and are performed parallel to the wound margin. Galeal releasing incisions are generally placed 1 to 2cm apart.
•Deep suture placement must include the galea in the suture path for maximal tissue-holding properties.
•Proposed scalp incisions are based on the ability to encompass the greatest vascular supply and maintain hairline position, with less consideration given to the direction of relaxed skin tension lines.
•Primary closure in hair-bearing areas should only be used if low tensions are generated. Higher tensions can cause telogen effluvium or, less commonly, permanent hair loss.
•Primary closure for large defects in non-hair-bearing areas can be used with favorable cosmetic outcomes.
•Primary closure of large defects in non-hair-bearing areas can be aided by the use of pulley sutures. In hair-bearing areas, the use of pulley sutures can cause telogen effluvium or, less commonly, permanent hair loss.
•Purse-string suture closures are best employed in non-hair-bearing scalps. Purse-string and pulley sutures can be combined with second intention healing.
•Skin grafts require a placement on a base of periosteum and loose alveolar tissue to survive.
•Skin grafts will leave a larger contour deformity when compared to second intention healing.
•For large rotation flaps, incise incrementally, and then complete hemostasis before incising further. This increases control and visibility.
•Rotation flap arclengths must be designed at least four times longer than defect diameter to prevent necrosis at the flap edge and possible hair loss.
•Reduced elasticity and mobility of scalp skin limits the use of transposition and advancement flaps.
•Larger scalp defects may require combinations of second intention, rotation flap(s), and skin grafts.
•Small to moderate standing cones can be sutured out using rule of halves or allowed to settle spontaneously.
5.1 Relevant Anatomy
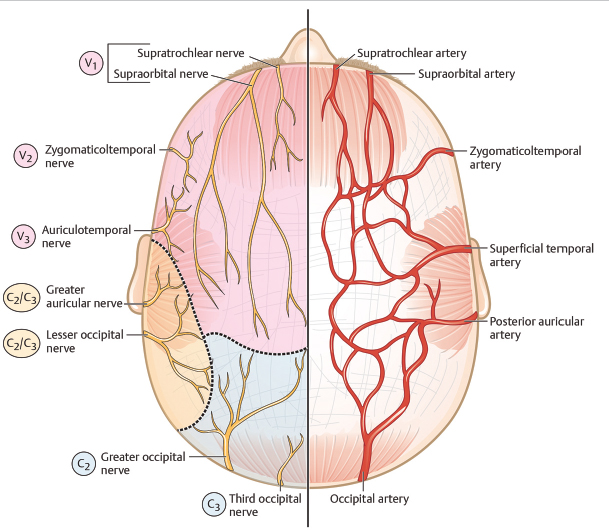
The cutaneous topography of the scalp relates to the underlying musculoskeletal framework (see Fig. 5.1). This framework determines scalp thickness and laxity and thus impacts strongly on reconstructive choices. Each topographic subunit of the scalp will have prominent neurovascular bundles originating peripherally, and coursing toward the scalp vertex. Anatomic knowledge of the position and plane of these bundles (as outlined later) helps direct flap design to maximize flap vascularity and minimize sensory changes. Reducing damage to terminal hairs requires careful consideration of incision angles to match hair follicle angles. In addition, undermining planes should be below hair bulbs, cautery has to be precise, and flap-closing tensions minimized to prevent permanent traction or scarring alopecia. Understanding all these variables inherent in scalp anatomy is required to optimize surgical outcomes.
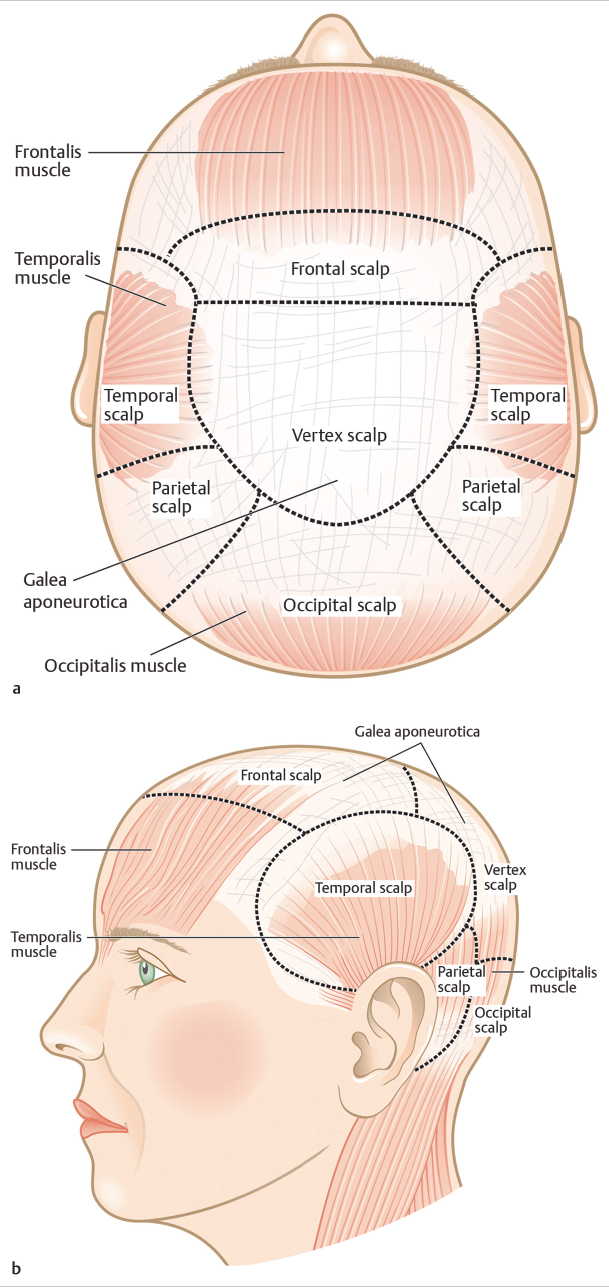
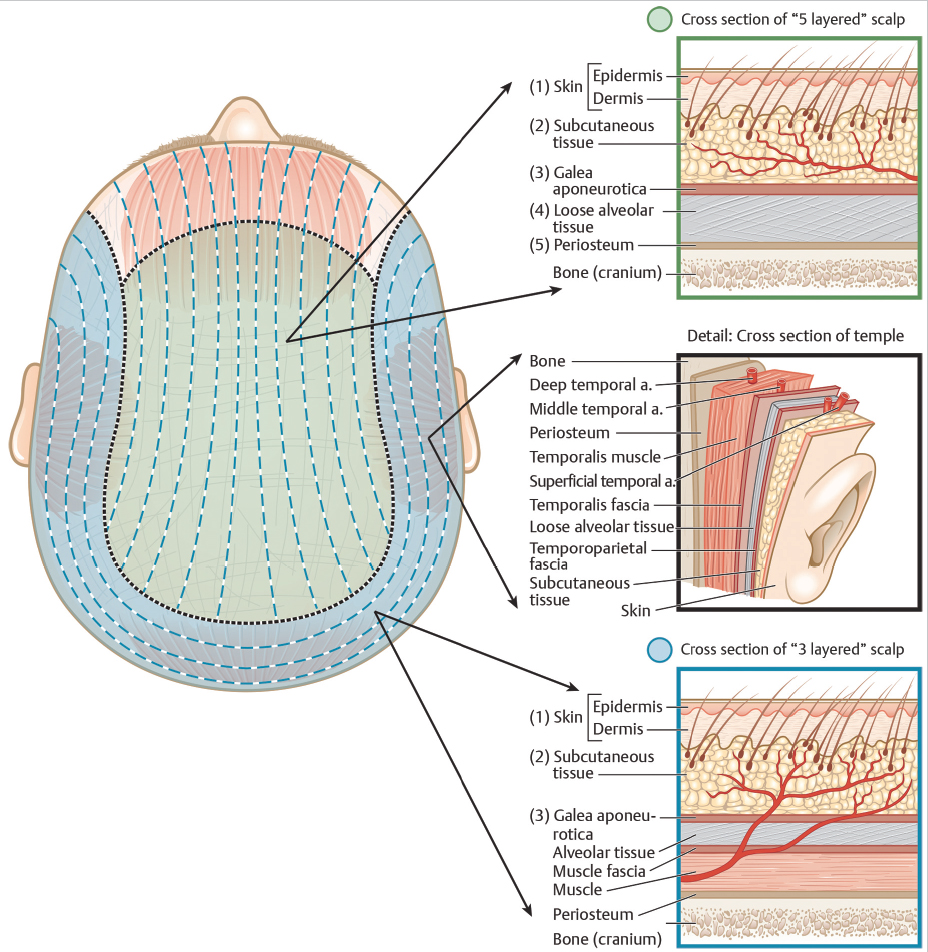
The scalp comprises five tissue layers, with exceptions at the lateral and posterior peripheries, where three layers can be defined (Fig. 5.2). The five layers, from superficial to deep, are: (1) skin, (2) subcutis, (3) galea aponeurotica, (4) loose connective fibroareolar tissue (subgaleal tissue/space), and (5) periosteum (pericranium). The presence of the subgaleal space, and the genetically determined degree of loose connective tissue within this space, allows the scalp to be a relatively glideable/mobile organ. However, at the posterior and lateral limits of the scalp, the absence of the subgaleal space restricts mobility. In these scalp areas, only skin, subcutis, and deep fascia are present.1 The limits of galea extension are the occipitalis muscle posteriorly, the temporalis fascia laterally, and the frontalis and orbicularis oculi muscle anteriorly. The anterior extension of the galea allows both the frontal scalp and forehead to move as a unit and can account for periorbital ecchymosis sometimes seen after frontal scalp surgery. The five scalp layers are discussed in greater detail in the following sections.
5.1.1 Skin
The scalp skin, comprising epidermis and dermis, is a bit of a paradox from a surgical perspective. While the skin is thicker than anywhere else on the head and neck,2 ranging from 3 mm on the vertex to 8 mm at the occiput, the structural integrity of the dermis is fairly friable, and consequently, does not hold deep sutures well. This necessitates that, if possible, placement of the deep sutures should include the more structurally robust galeal layer in the suture path. Dermal thickness varies according to patient age, ethnicity, and degree of actinic damage. Younger, sun-protected, Asian- or African-descent patients generally will have a thicker dermis. Langer’s lines relate to collagen bundles arranged in the dermis, aligning with creases, and coinciding with lines of minimum tension.3 On the scalp, they are mostly vertically longitudinal, until the occiput, where they become horizontal and circumferential (Fig. 5.2). Although orientating incisions along Langer’s lines can reduce closing tensions and scar width, location of scalp laxity and vascular bundles are generally more important variables to consider in flap design. Terminal hair follicles exit scalp skin at various angles according to location: almost horizontal over the central frontal scalp, sharply angled inferiorly at the scalp periphery, and more vertical as the vertex is approached. Hair bulbs are located at the dermal–subcutis junction averaging 4 to 6 mm below the skin surface. Minimizing hair follicle damage requires trichophytic incisions (the incision parallels the directional angle of the hair) and choosing an undermining plane below hair bulbs (deep subcutis or subgaleal). Careful attention to these variables avoids hair follicle transection and facilitates the narrowest possible scar with less chance of any ingrown hairs or cysts.
5.1.2 Subcutis
The subcutaneous fat is the second layer in the scalp. This layer is thick and houses a rich network of anastomosing arteries, veins, lymphatics, and coursing sensory nerves (Fig. 5.3). The neurovascular and lymphatic supply to the scalp is centripetal (i.e., larger trunks run from the periphery medially and toward the center, becoming smaller and anastomosing), subcutaneous, and similar in distribution. Their distal ends are attached to the deep layers of the dermis at the subcutis junction. The rich vascular network at this level is responsible for what can be significant scalp hemorrhage after only superficial wounds.1 The vascular supply is the anastomosed network between branches of external and internal carotid arteries. Where the scalp has five layers, there are no musculocutaneous perforators, and thus, a flap design that transects a significant portion of the peripheral vasculature can reduce flap tip perfusion and increase necrosis risk. Of note, the vascularity and relative perfusion of central scalp is decreased in male-patternbaldness,4 presumably related to the association between relative tissue hypoxia and hair loss. This may partially explain why surgery on bald scalp is usually less bloody than in patients who have no hair loss. Surgeons must be mindful that arterioles can be closely apposed to hairbulbs. Consequently, hemostasis has to be judicious and precise to reduce collateral damage to hair follicles and lessen the potential for permanent scarring alopecia. Sensory nerves in the subcutis have a similar course to that of the vascular system and peripheral incisions for flap design can transect larger nerve trunks resulting in sensory changes that can take an extended time to resolve. Rarely, sensory changes can be permanent. Lymphatics bear the same “snakelike” distribution, lying deep in the subcutaneous tissue. The dense network of lymph-collecting vessels arises from precollectors within 2 cm of the midline and runs obliquely down and backward to reach the first-tier lymph nodes. On average, four frontal-collecting, six parietal-collecting, and six occipital-collecting lymph vessels are found in the scalp.5
5.1.3 Galea Aponeurotica
Galea, the third layer in the scalp, is a 1- to 2-mm-thick, very dense, inelastic fibrous sheet. It is stretched under tension between the frontalis muscle anteriorly, moving over the vertex and extending to the occipital muscle posteriorly. The frontal and occipital muscle bellies are inserted directly into the galea. It fades out laterally by blending with the temporal fascia (Fig. 5.2).1 The frontalis muscle arises from the front of the aponeurosis and is inserted into the superior part of the orbicularis oculi. This allows the subaponeurotic/subgaleal space to extend anteriorly beneath the orbicularis oculi into the eyelids, yielding an effective dissection plane. As outlined earlier, this plane allows anterior and inferior movement of surgical blood, leading to periorbital ecchymosis and swelling. The fibrous nature of the galea imparts three important qualities. First, the high-tensile strength allows the galea to support buried or pulley sutures under very high tension. If galea is not captured in a suture path, closure of moderate- to high-tension reconstructions becomes difficult. Second, because the galea is stretched under tension between the frontal and occipital poles, an incision made in the galea can lead to retraction away from the wound edge. Surgeons must be mindful of this concept and ensure their suture path is angled to include the galea should retraction be evident. Third, as galea is significantly resistant to stretching, a practice of galeotomy, or linear galeal transection (serial relaxing incisions), is still used to reduce scalp tension and facilitate greater stretch.6 The effectiveness of galeotomies in reducing closure tension remains debated. In addition, galeotomies can increase the risk of vascular damage. In the author’s practice, galeotomies have given only minimal additional tissue length and are used only rarely in an attempt to gain maximal tissue length when reconstructions are under very high tension.
5.1.4 Subgaleal Loose Connective Tissue
The loose fibroareolar tissue makes up the fourth layer and presents as a potential space underneath the densely packed scalp layers above. This layer allows for the overlying scalp to glide over the periosteum and accounts for scalp movability. In scalps where this layer is well developed and relatively “thick,” the gliding phenomenon can be generous, while scalps that have a relatively poorly developed fibroareolar layer are found to be “tight.” The subgaleal space is avascular and easily separated by blunt dissection. As such, it presents the primary plane for scalp undermining. The extent of subgaleal loose connective tissue is the most important factor that determines scalp laxity and the ease with which scalp tissues can be moved during reconstructions.1 To a lesser degree, scalp laxity is accounted for by the ability of scalp to elasticize, which relates to its pliability along the Langer’s lines.
5.1.5 Periosteum
Periosteum (pericranium) is the fifth layer of the scalp and covers all the skull bones. It is a dense fibrous sheet, readily separable from the overlying loose subgaleal space, but relatively adherent to the underlying skull. However, periosteal stripping is possible, bloodless, and can be accomplished with blunt dissection. The periosteum is untethered from the bone in a rolling fashion using a periosteal elevator or equivalent. The minimal blood supply to periosteum comes from tiny bone perforators derived from meningeal vessels. During dissection, any bleeding is controlled with careful and precise cautery. Periosteal “toughness” allows consideration to suspend heavy or high-tension flaps from this dense layer in order to avoid widened scars. Although placement of periosteal supporting sutures is possible, the authors rarely practice this technique. Of note, the top layer of the skull, the outer table, just deep to the periosteum is often removed when a tumor is not able to be cleared within the periosteum or margins are not contiguous enough to be confident in tumor clearance.
5.2 Reconstructive Options
5.2.1 Algorithm for Scalp Reconstruction
Many author groups have published effective algorithms for scalp reconstruction.7,10 The presented algorithm represents the author’s primary decision pathway when deciding on a reconstructive choice in an outpatient setting using local anesthesia. Four components populate the author’s algorithmic approach. This includes defect size, which in the author’s experience can be divided into small (<2 cm in longest dimension assuming a circular defect;Fig. 5.4), moderate (3–5 cm in longest dimension;Fig. 5.5), and large or extensive (>6 or 9 cm in longest dimension, respectively;Fig. 5.6). Scalp tension/scalp mobility, which can be both site and patientdependent, has been separated into high, moderate, or low. The potential for a reconstruction to distort hairline position and the location of the defect in hair-bearing or alopecic scalp comprise the final two decision pathways. As previously outlined, patient and surgeon preferences can lead to a chosen reconstruction, which was not within the algorithmic outline.
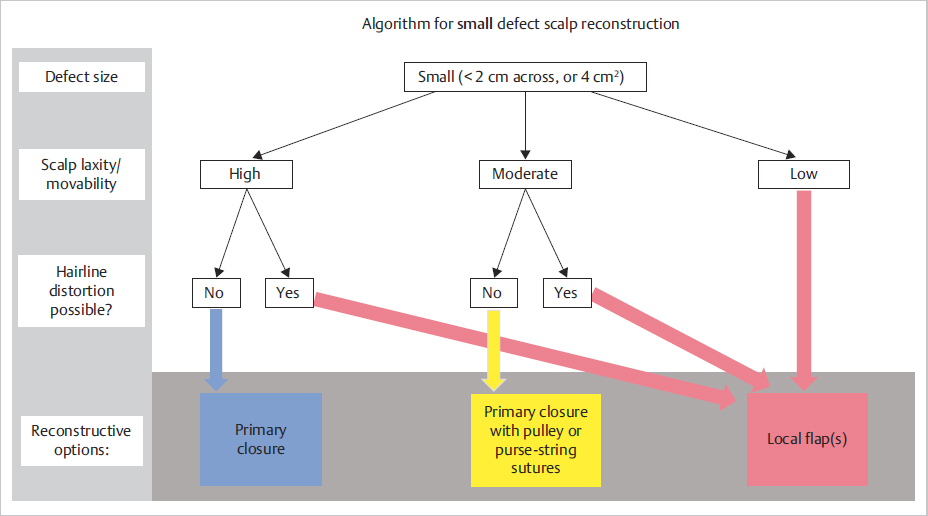
Fig. 5.4 Algorithm for reconstruction of small flap defects. The algorithm must be implemented in accordance with individual patient factors. Further information is found in the chapter text.
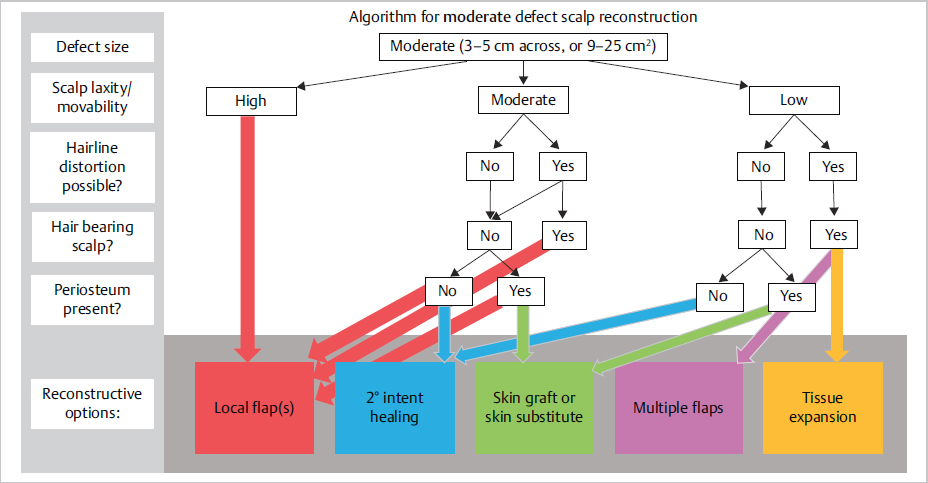
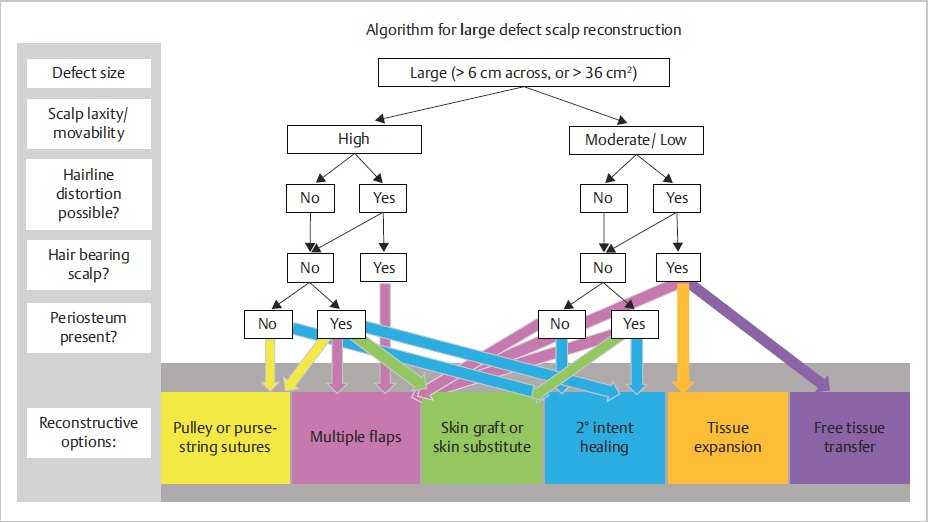
Fig. 5.6 Algorithm for reconstruction of large flap defects. The algorithm must be implemented in accordance with individual patient factors. Further information is found in the chapter text.
5.2.2 Second Intention Healing
Second intention healing (SIH) is a valuable scalp reconstructive option in a diffuse range of defect scenarios. The prevalence of SIH in scalp reconstruction is unknown. A British study estimated overall SIH prevalence at 41/1,000 population,11 while a U.S. private Mohs micrographic surgery center repaired 37.9% of wounds (at variable sites) using SIH.12 In the senior author’s (DMZ) practice, 15% of scalp defects are repaired with SIH. An interesting survey study found that the most experienced surgeons were significantly more likely to heal deep and larger wounds secondarily.13 The use of SIH as a reconstructive option remains very physician and institution dependent as evidenced by a systematic review7 where SIH was part of a reconstructive ladder, but not listed as surgical option in a 105-patient, single-institution study.14 The editors find SIH to be ideal for partial-thickness defects or shallow full-thickness defects in non-hair-bearing locations.
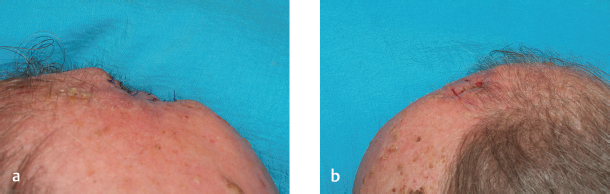
The ideal scalp sites for SIH are areas of alopecia, away from hairlines, with an intact periosteum, although any area of the scalp can be considered.15 Hair-bearing areas can be repaired with SIH, if the patient is less cosmetically concerned, or is willing to change their hairstyle to allow camouflage of the hairless scar. SIH over areas of absent periosteum or compromised vascular supply has been well documented.16,17 The authors have successfully used SIH in over 30 cases where periosteum was absent, including 1 case in a previous radiotherapy field. No infections occurred within the surrounding soft tissue or bone, and the postoperative course was well tolerated by patients. One additional case did not heal after 15 months, leading to sequestration of the outer table, requiring removal, and placement of a split-thickness skin graft (STSG).
The primary criterion that must be met before choosing SIH is the need for the patient and/or family member to care for an open, potentially draining wound, for a prolonged period of time. A study of 38 patients with a mean area of exposed soft tissue of 15.75 cm2 and mean area of exposed bone of 10.74 cm2 showed a mean time to epithelialize of 7 and 13 weeks, respectively.16 These parameters do not mirror the authors’ experience. In our patient population, time to complete healing with periosteum present averaged 14 weeks, and with periosteum absent 24 weeks (Fig. 5.7, Fig. 5.8). The authors’ mean size of scalp defect with periosteum present was 40.8 cm2, while mean size of defect with periosteum absent was 54.5 cm2. These larger defects partially explain the authors’ longer healing times. However, SIH is not linear, and larger wounds can heal quicker than expected given logarithmic wound contraction.18 Differences in wound care protocols, or patient factors, may also have played a role. Longer healing times for SIH compared to other reconstructive options can delay postoperative adjuvant therapy should this be required.